Hemodialysis access
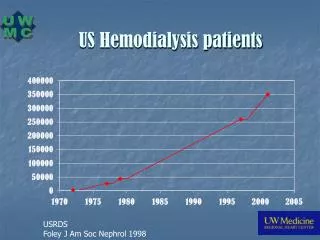
Hemodialysis access. Hemodialysis access. The number of patients with end-stage renal disease (ESRD) in the United States has increased steadily. 2030: 2.24 million patients with ESRD.

Hemodialysis access
E N D
Presentation Transcript
Hemodialysis access • The number of patients with end-stage renal disease (ESRD) in the United States has increased steadily. • 2030: 2.24 million patients with ESRD. • The creation and maintenance of functioning vascular access, along with the associated complications, constitute the most common cause of morbidity, hospitalization, and cost in patients with end-stage renal disease.
Vascular Access via Percutaneous Catheters • useful method of gaining immediate access to the circulation. • associated with higher risks. • the use-life of this type of access is shorter than that of AVFs. • Noncuffed catheters • Short term: <3 weeks
Cuffed catheters Patients who will require long-term access should have a tunneled catheter placed. allow so-called no-needle dialysis with high flow rates eliminate the problem of vascular steal placed in a subcutaneous tunnel under fluoroscopic guidance Vascular Access via Percutaneous Catheters: cuffed catheters
Vascular Access via Percutaneous Catheters: cuffed catheters • The Dacron cuff allows tissue ingrowth that helps reduce the risk of infection when compared with noncuffed catheters.
Hemodialysis access: complications • Complications can be divided into those that occur secondary to catheter placement and those that occur later. • The early complications of subclavian or internal jugular placement include pneumothorax, arterial injury, thoracic duct injury, air embolus, inability to pass the catheter, bleeding, nerve injury, and great vessel injury.
Hemodialysis access: complications • A chest radiograph must be taken after catheter placement to rule out pneumothorax and injury to the great vessels and to check for position of the catheter. • The incidence of pneumothorax is 1% to 4%,the incidence of injury to the great vessels is less than 1%. • Thrombotic complications occur in 4% to 10% of patients • Infection may occur soon after placement (3 to 5 days) or late in the life of the catheter and may be at the exit site or the cause of catheter-related sepsis. • Rate of infection between 0.5 and 3.9 episodes per 1000 catheter-days. • Catheter thrombosis increases the incidence of catheter sepsis.
Vascular Access via Arteriovenous Fistulas • The ideal vascular access • permits a flow rate that is adequate for the dialysis prescription (³ 300 ml/min), • can be used for extended periods, • and has a low complication rate. • The native AVF remains the gold standard
Arteriovenous fistulas • The standard by which all other fistulas are measured, is the Brescia-Cimino fistula. (2 year patency: 55% to 89%) • radial branch-cephalic direct access (snuffbox fistula), • autogenous ulnar-cephalic forearm transposition, • autogenous brachial-cephalic upper arm direct • access (antecubital vein to the brachial artery), • autogenous brachial-basilic upper arm transposition (basilic vein transposition). These options should be exhausted before nonautogenous material is used for dialysis access.
Noninvasive Criteria for Selection of Upper-Extremity Arteries and Veins for Dialysis Access Procedures
radiocephalic fistula (anatomic snuff-box) • radiocephalic fistula (Brescia-Cimino)
Vascular access via AVFs: • brachiocephalic fistula • brachiobasilic fistula
Arteriovenous fistulas: Complications • Failure to mature • Stenosis at the proximal venous limb (48%). • Thrombosis (9%) • Aneurysms (7%) • Heart failure • The arterial steal syndrome and its ensuing ischemia occur in about 1.6%: pain, weakness, paresthesia, muscle atrophy, and, if left untreated, gangrene • Venous hypertension distal to the fistula : distal tissue swelling, hyperpigmentation, skin induration, and eventual skin ulceration.
Prosthetic Grafts for vascular access • Upper arm grafts have a high flow rate and a low incidence of thrombosis. • higher incidence of ischemia in the hand • higher rate of stenosis, sec to endothelial hyperplasia.
Options for treating steal DRIL procedure distal revascularization-interval ligation excision of a portion of the vein plication w/ mattress or continuous sutures crossed PTFE band interposition of a 4 mm PTFE
Venous angioplasty Graft thrombolysis Treatment of venous access complications.
Contraindications to Thrombolytic Therapy • Absolute Recent major bleeding Recent stroke Recent major surgery or trauma Irreversible ischemia of end organ Intracranial pathology Recent ophthalmologic procedure • Relative History of gastrointestinal bleeding or active peptic ulcer disease Underlying coagulation abnormalities Uncontrolled hypertension Pregnancy Hemorrhagic retinopathy
Hemodialysis access • Quality of life and overall outcome could be improved significantly for hemodialysis patients if two primary goals were achieved: • Increased placement of native AVFs: a minimum of 50% of new dialysis patients should have primary AVFs. • Detection of dysfunctional access before thrombosis of the access route occurs. National Kidney Foundation Dialysis Outcome and Quality Initiative (NKF-DOQI)