Download
1 / 34
360 likes | 783 Vues
Rickettsia, Orientia, Ehrlichia and Coxiella. Rickettsia Rocky Mountain spotted fever Rickettsialpox Epidemic and sporadic typhus Oral: Vesicles in the oral cavity - R. akari Macular rash, swollen tissue - R. rickettsii Orientia Scrub typhus Ehrlichia Ehrlichiosis

E N D
Rickettsia, Orientia, Ehrlichia and Coxiella Rickettsia Rocky Mountain spotted fever Rickettsialpox Epidemic and sporadic typhus Oral: Vesicles in the oral cavity - R. akari Macular rash, swollen tissue - R. rickettsii Orientia Scrub typhus Ehrlichia Ehrlichiosis CoxiellaQ fever
Rickettsia, Orientia, Ehrlichia and Coxiella Aerobic, Gram-negative bacilli (but stain poorly) Obligate intracellular parasites Coxiella & Ehrlichia multiply in vacuoles Rickettsia and Orientia are found free in the cytoplasm Utilize the host cell's ATP, coenzyme A and NAD as long as they are available
Rickettsia, Orientia, Ehrlichia and Coxiella Proliferate at the site of infection The organisms eventually lyse the cell Spread to the endothelial cells lining small blood vessels Focal hyperplasia, inflammation Formation of microthrombi, with localized infarction of organs and tissues
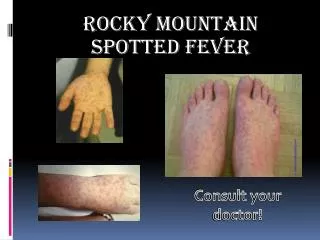
Rickettsia rickettsii Can grow in the nucleus Causes Rocky Mountain Spotted Fever Damages endothelial cells and causes leakage of blood vessels Transmitted by wood ticks, dog ticks or Lone Star ticks Incidence highest in children and teenagers Abrupt onset: Fever, chills, headache, myalgia
Rickettsia rickettsii Macular rash on hands, wrists, feet and ankles, then covers the entire body Sometimes found on oral mucosa Causes swollen throat and tongue Complications: splenomegaly, neurologic disturbances, thrombocytopenia, disseminated intravascular coagulation, and heart failure Mortality is 20% if not treated
Rickettsia prowazekii Causes Epidemic Typhus (louse-borne typhus) Associated with crowded, unsanitary conditions that favor the spread of body lice Abrupt onset, with fever, chills, myalgias, and severe headache Maculopapularrash develops on day 5 and spreads Complications: myocarditis, CNS dysfunction. Mortality can be as high as 60% if untreated.
Orientia tsutsugamushi Causes Scrub typhus Fever develops suddenly, and increases to 104°F in a few days A macular to papular rash develops on the trunk in less than half the cases Generalized lymphadenopathy, splenomegaly, CNS complications and heart failure can occur The viral load of HIV patients is lower if they are also infected with O. tsutsugamushi
Rickettsia akari Causes rickettsialpox Papular skin lesion at the site of the mite bite (mouse mite), lymphadenopathy, fever, chills, headache, and a generalized papulovesicular rash In some cases vesicles develop on the palate, tongue, buccal mucosa, pharynx and lips.
Ehrlichia Infectlymphocytes, neutrophils monocytes, and capillary endothelial cells High fever, malaise, headache and myalgia Only 20% of the patients present rashes (thus difficult to diagnose)
Coxiella burnettii Resistant to desiccation, and can remain in the environment Q fever is most commonly caused by inhalation of airborne particles Proliferates in the respiratory tract, with subsequent dissemination
Coxiella burnettii In severe cases it may cause necrotizing hemorrhagic pneumonia The most common clinical manifestation is endocarditis Sudden onset with severe headaches, high-grade fever, chills and myalgias Respiratory symptoms are generally mild, but can be severe.
Treatment and Prevention Tetracycline and chloramphenicol Prompt diagnosis and initiation of therapy results in good prognosis Vaccines are available against epidemic typhus and Q fever Hygiene, and de-lousing sprays can control the human body louse
Chlamydiae They were initially thought to be viruses since they are small enough to pass through 0.45 µm filters and are obligate intracellular parasites They have an inner & outer membrane, like Gram-negative organisms, but no peptidoglycan layer and no muramic acid Cause psittacosis, trachoma and lymphogranuloma venereum
Chlamydiae They exist in 2 morphologically distinct forms: 1. Extracellular, infectious elementary body (300-400 nm) 2. Intracellular, metabolically active, replicating, but non-infectious, reticulate body (800-1000 nm)
Chlamydiae Chlamydia replicate in phagosomes, forming an inclusion The intact cell envelope inhibits phagosome-lysosome fusion If the outer membrane is damaged or the chlamydiae are heat-inactivated or coated with antibodies, phagolysosome fusion proceeds
Chlamydia trachomatis Infects epithelial cells of mucosal surfaces: conjunctivae, endocervix, urethra, rectum, endometrium, fallopian tubes, respiratory tract and conjunctivae The lymphogranuloma venereum (LGV) biovar infects lymphoid tissue and replicates in mononuclear phagocytes Trachoma strains infect epithelial cells Clinical manifestations arise from cell destruction and the host inflammatory response Granuloma formation is typical
Chlamydia trachomatis Infection leads to formation of antibodies and cell-mediated immune reactions but not to resistance to reinfection or elimination of the organism Re-infection induces a vigorous inflammatory response with subsequent tissue damage This response produces the vision loss in patients with eye infections, and scarring with sterility and sexual dysfunction in patients with genital infections
Chlamydia trachomatis C. trachomatis is the one of the most common sexually transmitted bacteria in the US (4 million new cases per year) It is estimated that 50 million new cases occur per year worldwide Most urogenital infections in women are asymptomatic, but may become symptomatic
Chlamydia trachomatis Clinical syndromes include cervicitis endometritis urethritis salpingitis pelvic inflammatory disease (PID) 1 million women/year in the US Can cause scarring of fallopian tubes, preventing fertilization Most genital infections in men are symptomatic
Chlamydia trachomatis Treatment and Prevention Ocular and genital infections in adults One dose of azithromycin doxycycline for 7 days ofloxacin for 7 days Sanitation is important in areas where trachoma is endemic Neonatal conjunctivitis: Erythromycin for 10-14 days.
Chlamydophila psittaci Transmitted to humans from infected birds via the inhalation of dried bird excrement Spreads to the liver, spleen, lungs; causes lymphocytic inflammation, edema, thickening of the alveolar wall, infiltration of macrophages
Chlamydophila psittaci Causes psittacosis (parrot fever) characterized by headache, high fever and chills. Other symptoms may include malaise, anorexia, myalgia, arthralgia, nonproductive cough Infections are treated with tetracycline and erythromycin
Chlamydophila pneumoniae First isolated from the conjunctiva of a child in Taiwan, and was initially considered to be a psittacosis strain It was found to be serologically related to strain AR, which led to the designation “TWAR strain” DNA homology studies have indicated that it is a species distinct from both Chlamydia trachomatis and Chlamydia psittaci
Chlamydophila pneumoniae Transmitted by respiratory secretions Causes pneumonia, bronchitis, pharyngitis, sinusitis and flu-like illness Most common in the age group 60-79
Chlamydophila pneumoniae C. pneumoniae infection is strongly associated with coronary artery disease atherosclerosis of the carotid artery, aorta, and peripheral arteries C. pneumoniae in atherosclerotic plaque
Chlamydophila pneumoniae Treatment Macrolides (erythromycin, azithromycin, clarithromycin) before identification of the cuase of pneumonia Doxycycline or levofloxacin administered for 10-14 days