Download
1 / 56
560 likes | 679 Vues
This toolkit, developed by Troutman Sanders LLP for the Virginia Department of Health, serves as a comprehensive guide for hospitals to create an effective operational infrastructure in response to critical resource shortages. It is designed as a companion to the Hospital Implementation Guide, providing facilitators with presentations and customized instructions tailored to their specific audiences. The toolkit includes protocols for resource allocation, communication plans, and ethical frameworks, ensuring preparedness for emergency situations while emphasizing the importance of review and adaptation.

E N D
OPERATIONAL INFRASTRUCTURE [ENTER FACILITATOR’S NAME AND CONTACT INFORMATION] Developed by Troutman Sanders LLP Developed for the Virginia Department of Health Funded by Centers for Disease Control and Prevention
Toolkit Presentations Instructions for Use • Toolkit Presentations are intended to be a companion to the HospitalImplementation Guide and should not be used in isolation. • The Presentations are intended to serve as a starting point for the facilitator. The facilitator should thoroughly review the Presentation prior to use in Implementation Team, CRAG or Subcommittee meetings and customize the Presentation to meet the unique needs of the meeting participants. • Pay particular to attention to the information provided in brackets ([ ]), which must be completed by the facilitator prior to use. • Included in the “Notes” section of each slide are the following types of information: • Slide Type, which indicates whether the slide is for information or discussion, serves as a placeholder, or is some combination thereof • Planning Guide Section(s), which will direct the facilitator to the corresponding sections of the Planning Guide and HospitalImplementation Guide for further information • Special Instructions, which provides directions for the facilitator to customize the slide for the intended audience • Speaker’s Notes, which provides more detailed information to supplement the material on the slide • Refer to the Hospital Implementation Guide for further guidance and helpful hints on effectively completing the process described in the Planning Guide.
CRAG Members • [Enter names and departments of each CRAG member]
Add slides from Altered Standards Overview and/or Chapter 1 presentation, as needed, to re-introduce the CRAG to the concept of altered standards and critical resource shortage response planning, especially if new members are involved.
Why do we need an Operational Infrastructure? • Many hospitals already have an emergency response infrastructure • Most hospitals do NOT have the type of infrastructure that will be needed to respond to a critical resource shortage event • An overall operational infrastructure will provide consistency to Protocol development, implementation, and operationalization
Chapter Overview • Determine process for activation and termination of the CRSRP • Determine process for activation and termination of each Protocol • Develop structure for making resource allocation decisions • Develop infrastructure for reviewing and revising CRSRP during a CRSE • Define “essential documentation”
Chapter Overview cont. • Develop process for responding to non-compliance • Identify resources for psychological and emotional support • Develop a communication plan • Develop strategy for providing palliative care during a critical resource shortage event • Determine goal • Develop standard definition • Identify mechanisms for providing palliative care
Education & Communication Protocol Protocol Protocol Protocol Protocol Protocol Protocol Protocol Building the CRSRP Strong Foundation Ad Hoc Operational Infrastructure Ethical Framework
Operational Infrastructure Ethical Framework [Withdrawal/Withholding] of Resources [Exclusion Criteria] [LOW PRIORITY ETHICAL VALUE] [LOW PRIORITY ETHICAL VALUE] [LOW PRIORITY ETHICAL VALUE] [LOW PRIORITY ETHICAL VALUE] [LOW PRIORITY ETHICAL VALUE] [MEDIUM PRIORITY ETHICAL VALUE] [MEDIUM PRIORITY ETHICAL VALUE] [MEDIUM PRIORITY ETHICAL VALUE] [MEDIUM PRIORITY ETHICAL VALUE] [MEDIUM PRIORITY ETHICAL VALUE] [HIGH PRIORITY ETHICAL VALUE] [HIGH PRIORITY ETHICAL VALUE] [HIGH PRIORITY ETHICAL VALUE] [HIGH PRIORITY ETHICAL VALUE] Ethical Framework [INSERT GOAL DEVELOPED IN SECTION 3.2]
What’s Next? Development of the operational infrastructure Operational Infrastructure Ethical Framework
CRSRP Process Activation Implementation Maintenance Termination
Activation of CRSRP Supply of Critical Resources CRSE Normal Demand for the Resource
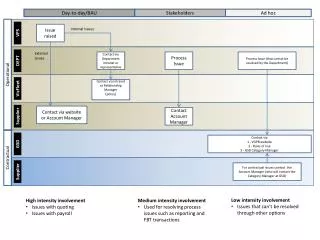
Activation Flow Chart Event Occurs Resource levels begin to diminish & demand increases Who is responsible for each step in the activation process? Identify Critical Resource Shortage Event Report Critical Resource Shortage Event Declare Critical Resource Shortage Event Activate CRSRP
Identifying a Critical Resource Shortage Event DURATION For how long will demand exceed supply? STATUS Does demand exceed supply? MITIGATION Options for obtaining additional supplies of the resource. FORECAST When will demand exceed supply if it doesn’t already? MAGNITUDE To what extent does or will demand exceed supply?
Declaration and Activation CRSE Normal Who will declare the CRSE? Demand for the Resource Who will activate the CRSRP? Supply of the Resource
Governmental Emergency Declarations • How will federal, state or local emergency declarations be identified? • Who will find, read and summarize the declaration(s)? • What is the role of legal counsel?
CRSRP Termination Not soon enough Too soon
Activation of Protocols CRSE Normal Demand for the Resource Supply of Critical Resources
Simultaneous Activation CRSE Normal Demand for the Resource Supply of Critical Resources
Asynchronous Activation CRSE Normal Demand for the Resource Supply of Critical Resources
Protocol Termination Options • Simultaneous • Asynchronous • Who will terminate the Protocols? • Will the decision vary by Protocol? • What information is required? • Termination by Tier
Model 4 Triage Officer and Triage Committee INELIGIBLE Resource #1 Resource #2 ELIGIBLE ED Inpatients INELIGIBLE DirectAdmits
Reassessment of CRSRP Re-assessment of situational factors Implementation of CRSRP Dissemination of CRSRP Revision of CRSRP
Documenting CRSRP Modifications Re-assessment of situational factors Revision of CRSRP
Primary Functions of Documentation During a CRSE • Care and safety of patients • Support Protocols • Quality assessment • Obtain timely reimbursement How will you ensure the completion of “essential documentation”? Essential Documentation
Reasons for Non-Compliance That is outside my scope of practice. My patient, my responsibility, my decision. My patient deserves to receive the resource. I won’t do that because I don’t want to get sued. The triage committee used the Protocol incorrectly. I don’t have the knowledge or skills to successfully complete this task.
Non-Compliant Providers How will you respond? Ignore Counseling/ Persuasion Directive Assume control of patient Restrict/ suspend privileges Terminate employment/ revoke privileges