Download
1 / 41
561 likes | 1.17k Vues
Treatment of Erectile Dysfunction. MODIFIED BY ISRAA OMAR. What is Erectile Dysfunction?. The persistent or recurrent inability to obtain or maintain an erection sufficient for sexual activity > 50% of men aged 40 – 70 will have fairly marked erectile problems

E N D
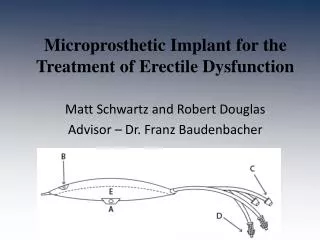
Treatment of Erectile Dysfunction MODIFIED BY ISRAA OMAR
What is Erectile Dysfunction? • The persistent or recurrent inability to obtain or maintain an erection sufficient for sexual activity • > 50% of men aged 40 – 70 will have fairly marked erectile problems • Incidence is on the rise due to aging population & and prevalence of other co-morbidities (i.e. diabetes, cardiovascular disease)
Men With ED • ED can have a major impact on the quality of life and self-esteem of men who suffer from it • Men often draw a link between their masculinity and their ability to have an erection • Some men with ED may begin to think that they are no longer a “real” man • This can lead also to affected relationships with partners
Pathophysiology: Mechanism of an erection • A normal erection relies on the coordination: • Vascular • Neurological • Hormonal • Psychological • An erection can occur following direct genital stimulation or auditory or visual stimulation, aspects that contribute to the influx of blood to the penis • An erection occurs when the amount of blood rushing to the penis is greater than the amount of blood flowing from it.
A massive influx of blood accumulates in the sinusoidal spaces due to relaxation of smooth muscle & dilatation of arteries corpora cavernosa to swell (tumescence) • Tumescence compresses the veins that normally drain the penis prevents blood outflow & maintains penile rigidity • Usually following ejaculation: • A reduction in arterial inflow due to contraction of the smooth muscle cells • Combination of increased venous return • loss of erection (detumescence)
Erectile Dysfunction • ED is most often an organic origin (up to 80%) • Can also have psychogenic causes • In several cases, it is both organic/psychogenic in origin mixed-type ED
1. Main Organic Causes • Vascular • Roughly 40% of cases of ED in men over 50 • Vascular problems can impede arterial blood flow into the penis • Examples: diabetes, cardiovascular disease (hypertension ,dyslipidemia), Peyronie’s disease, smoking, and trauma affecting blood circulation
Neurological conditions • Can lead to interruption in nerve impulse or the failure to conduct nerve impulses • Examples: diabetic or alcoholic neuropathy, MS, stroke, trauma or surgical procedures involving the spinal cord or pelvis • Hormone disorders • ED that is hormonal in origin can be related to low circulation blood levels of testosterone (hypogonadism), hyperprolactinemia (drug-related or non-drug related), hypothyroidism, adrenal insufficiency or glucocorticoid excess.
2. Psychogenic Origin • Can be cause by: • Anxiety • Depression or psychosis • Possibly with a loss of self-esteem • If causes of erectile dysfunction are completely psychological, the patient will continue to have nocturnal erections • Men with psychogenic ED often lose interest in sex
Drug-induced male sexual dysfunction.Pharmacist’s Letter/Prescriber’s Letter 2006; 22(9):220907.
Treatment Options • PDE5 Inhibitors • Sildenafil • Varedenafil • Tadalafil • Centrally Acting Oral Drugs • Apomorphine • Intraurethral suppositories • Alprostadil • Intraurethal gel • Penile injections • Vacuum devices
1. PDE5 Inhibitors • NO in the corpus cavernosum of the penis binds to guanylatecyclase receptors, which results in increased levels of cGMP, leading to smooth muscle relaxation (vasodilation) • Men who have erectile dysfunction often produce insufficient amounts of NO. • The small amount of cGMP produced is being broken down at the same rate, so they cannot maintain an erection. • Theses drugs work by selectively inhibiting PDE5, by binding with PDE5's active site. • This prevents the hydrolysis of cGMP to inactive GMP, allowing cGMP to accumulate and prolong the vasodilation effect, resulting in a stronger and longer erection. • All 3 drugs work regardless of the cause of ED, but all require sexual stimulation for activation.
The figure below shows the mechanism of action of Viagra, and the other PDE5 inhibitors, on the nitric oxide cycle.
Contraindications • Since PDE5 inhibitors may cause transiently hypotension, organic nitratesshould not be taken for at least 48 hours after taking the last dose. • Using organic nitrates within this timeframe may increase the risk of life-threatening hypotension.
2. Centrally Acting Oral Drugs • Apomorphine is a centrally acting drug that improves erectile dysfunction by enhancing the central natural erectile signals that normally occur in the brain during sexual stimulation. • It is a non-selective dopamine receptor agonist and acts mainly on dopamine D2-like receptors in the brain.
3. Intraurethral Suppository • Alprostadil • 250ug, 500ug, 1000ug • Prostaglandin E1 analogue which is a vasodilator • A choice for people: • Who do not respond to oral pills • Are afraid of injections • Suppository (about the size of a grain of rice) which is placed about 1 cm inside the urethra using a special applicator
Advantages • Gives an erection similar to penile injection therapy • Gives the most normal looking erection. • The head of the penis doesn’t swell in penile injections/PDE5 inhibitors but does with MUSE®
4. Intraurethal Gels • Gives an erection similar to penile injection therapy • Possibly stronger than using MUSE® • Must be kept in the fridge and has a 30 day expiry date • Many combinations • Dispense in 0.2ml single use syringes • Administer intraurethrally 10 – 15 minutes prior to sexual intercourse • Hold penis upright for 30 seconds to allow medication to absorb • Rub any excess cream over the forehead of the penis
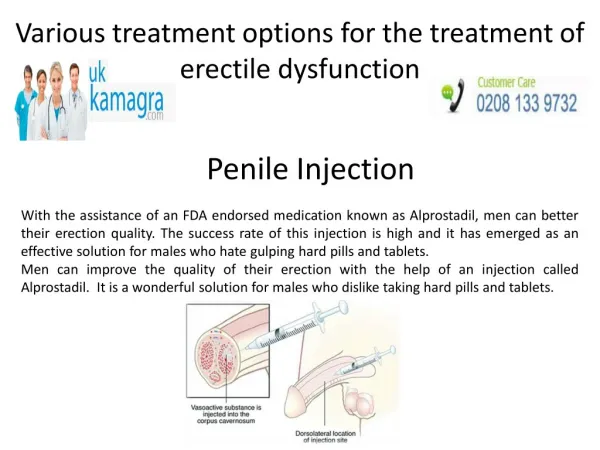
5. Penile Injections • Intracavernosal injection therapy • Very safe & highly effective • Around since 1983. • In 1982, a French surgeon injected a vasodilator into the pelvic artery & the patient obtained an erection • Shortly after, a British physician injected a drug directly into the penis
Alprostadil • Prostaglandin E -1 cAMP • Vasodilator & muscle relaxant of corpus cavernosum & trabecular smooth muscle • Prefilled syringe • Works in 60% men with ED • Will work better with milder erection problems • Can cause an aching or burning penile pain in some men • Papaverine • Inhibits phosphodiesterase in smooth muscle cells, which cAMP & cGMP relaxation of vascular smooth muscles
Phentolamine • Blocks -adrenergic receptors in penile blood vessels relaxation of trabecular cavernous smooth muscles & dilatation of the penile arteries • Weak erectile-promoting effect when used alone. • Potentiates the effect of papaverine or PGE-1 • Atropine • Smooth muscle relaxation • Chlorpromazine • blocker activity
6. Vacuum Devices • Erect penis (especially Caucasian) appears blue or grey • 50% of blood from arteries oxygenated • 50% of blood from veins non-oxygenated • 80-90%of men can obtain an erection • Overall patient satisfaction 60-80% • Some men will also have to trim the pubic hair to maximize seal
Vacuum Devices • Takes 2-10 minutes to obtain a functional erection • Take on average 4 attempts to use pumps to become proficient • Need to place constriction ring as close as possible to base of penis. • Penis will be hard on one side of ring and soft on the other side • Only wear for maximum 30 minutes • C/I: • Blood thinners or history of bleeding disorders • Diminished penile sensation • History of priapism
How to Use Vacuum Devices • Place the pump, which can be pumped by hand or run on batteries, over the penis. • Pump the air out of the cylinder so that a vacuum is created. The vacuum draws blood into the shaft of the penis and causes it to swell and become erect. • Once the penis is erect, with the help of lubricant, slide the retaining band down onto the lower end of the penis. • Remove the pump after releasing the vacuum.
OsbonErecaidConstriction Rings Pink = firm fit Beige = Regular fit Each colour comes in 2 sizes small and large
Actis Adjustable constriction loop
Female Sexual Dysfunction • Highest proportion occurs between the ages of 18 and 29. • Most women can reach orgasm when the clitoris is stimulated, but only about half of women regularly reach orgasm during sexual intercourse. • About 1 of 10 women never reaches orgasm.
The World Health Organization International Classifications of Diseases has divided Female Sexual Dysfunction into four disorders: • Desire disorder: a persistent absence of desire for sexual activity. • Arousal disorder: a persistent inability to attain or maintain sufficient sexual excitement. • Orgasm disorder, a persistent difficulty, delay or absence of orgasm after sufficient stimulation. • Pain disorder, persistent genital pain associated with sexual intercourse or stimulation
Causes of FSD • Arousal and orgasmic disorders can be caused by a lack of blood circulation to the clitoris and genital area and may be related to medical conditions such as: • Vascular disease • High blood pressure • Diabetes • Pelvic trauma • Use of certain drugs, including anticonvulsants, chemotherapy drugs, beta-blockers, and oral contraceptives, can also reduce the sex drive. • Drinking excessive amounts of alcohol.
A reduction in sex drive may result from depression, anxiety, stress, or problems in a relationship. • Fluctuations in the levels of estrogen and testosterone hormones, which occur monthly and during pregnancy, can affect sex drive. • Women who have undergone treatment for breast or ovarian cancer are at high risk for sexual dysfunction • Menopause: In postmenopausal women, sex drive may be reduced because estrogen levels decrease. Sex drive may also be reduced in women who have had both ovaries removed.
Testosterone • Most commonly used drug for treatment of FSD, especially in post-menopausal women. • Works to stimulate sexual desire. • Extremely low doses required- 20mg administered subcutaneously every three weeks. • Creams, patches, and combinations with estrogen and progesterone are being developed. • Side effects: masculinization and could cause liver toxicity in high doses. • Intrinsa is a Testosterone patch.
Estrogen (Premarin) • Available in pill, cream or injection • Used to help relieve menopause symptoms that occur due to decrease in levels of estrogen such as vaginal dryness, itching and discomfort. • Side effects of conjugated estrogens include headache, abdominal pain, nervousness, nausea, back pain, joint pain and vaginal bleeding. • Patients may also experience vaginal spotting, loss of periods or excessively prolonged periods, breast pain, breast enlargement and an increase or decrease in sexual drive.
Viagra and Befar for women… • Due to Viagra’s PDE5 inhibition it may improve vaginal engorgement and lubrication. • Viagra for women is called Avlimil and was created in 2003. • 84 percent success rate of decreasing symptoms of female sexual dysfunction, but It doesn’t have FDA approval yet. • Befar, the topical alprostadil cream, may be used to treat Female Sexual Arousal Disorder. It would cause clitoral stimulation by vasodilatation.