Sedative-Hypnotics
Teresita N. Avendano-Batanes, M.D., DPBA Department of Anesthesiology College of Mediciane UERMMMCI. Sedative-Hypnotics. Sedative - Hypnotics. Sedative Anxiolytic exerts a calming effect makes one less responsive to stimulation with decreased spontaneous activity Hypnotic

Sedative-Hypnotics
E N D
Presentation Transcript
Teresita N. Avendano-Batanes, M.D., DPBA Department of Anesthesiology College of Mediciane UERMMMCI Sedative-Hypnotics
Sedative - Hypnotics • Sedative • Anxiolytic • exerts a calming effect • makes one less responsive to stimulation with decreased spontaneousactivity • Hypnotic • encourages onset • maintains sleep • usually attained at higher doses of a sedative
Sedative - Hypnotics • Death • Coma A • Anesthesia B • Hypnosis • Sedation Increasing Dose • Drug A: older Sed.-hypnotics, e.g. Barbiturates • Drug B: greater margin of safety, e.g. benzodiazepines
Benzodiazepines • aryl-1,4-benzodiazepines • 7-position substituent: halogen or nitro-group • - required for sedative-hypnotic activity
Benzodiazepine • • Flumazenil (Anexate) – antagonist of benzodiazepine • • a synthetic benzodiazepine derivative
Benzodiazepines • for sedative-hypnotic activity • Diazepam (Valium) 4. substitution in the 7-position, such as with a halogen or nitro group is required Triazolam (Halcion) • Flurazepam (Dalmane) 5. Midazolam (Dormicum) • Lorazepam (Ativan) 6. Estazolam (Esilgan) • *Flumazenil (Anexate) – antagonist of benzodiazepine • MOA: competitive antagonism at the GABAA receptor • a synthetic benzodiazepine derivative
Barbiturates • Structure – Activity Relationships • 1. Substitution at C5 determines • a. Hypnotic potency: long-branched chain > short straight chain • b. Anti-convulasant activity: phenyl group is anti-convulsive • 2. Replacing O2 at C2 (Oxybarbiturate) with • S (Thiobarbiturate) • lipid solubility onset of action • 3. Short duration of action–methyl substitution at N1
Sedative-Hypnotics • Alcohols: Ethanol, Chloral Hydrate • Ethers • New Drugs:Other Drugs with • *Buspirone - anxiolytic Sedative Effects • * Zolpidem - hypnotic 1. Clonidine • * Zaleplon – hypnotic 2. Antipsychotic tranquilizeres 3. Tricyclic Antidepressants 4. Antihistamines
Benzodiazepines and Barbiturates • Pharmacokinetics • Routes of Admi/Absorption: po, rectal, IV, IM, SQ • Distribution • major role of lipid solubility to gain entry into CNS • thiobarbiturates more lipid vs. oxybarbiturates • rapid redistribution which termination CNS effects • all cross placental barrierneonatal depression • (+) in breast milk depression in breastfed babies • extensive protein binding: benzodiazepines: 60 – 90% • chloral hydrate displaces warfarin from plasma protein binding site anticoagulant effect of warfarin
Benzodiazepines • Biotransformation/Excretion • by microsomal drug metabolizing enzymes (liver)to water-soluble metabolites excretion via the kidneys • Table M. Some benzodiazepines with their metabolites:
Barbiturates • - inactive metabolites w/ few exceptions • *Phenobarbital – 20 – 30% excreted unchanged; elimination half-life of 4 – 5 days • multiple dosing cumulative CNS effects • biodisposition affected by hepatic changes due to: • old age, diseases, microsomal enzyme activity
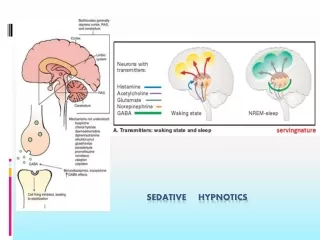
Benzodiazepines and Barbiturates • Pharmacodynamics • Mechanism of Action: bind • Benzodiazepines molecular components of • barbiturates*GABAA receptors in CNS opening of Chloride ion channels Chloride ion conductance • *Do not substitute for GABA but appear to enhance effects of GABA
Organ Level Effects • Sedation • may be with by euphoria, impaired judgement • anterograde amnesia – cannot recall events happening during the drug’s action (benzodaazepines) 2. Hypnosis • time to fall asleep is , duration of stage 2 NREM sleep is ; duration of REM sleep is • use of sedative-hypnotics for > 1 – 2 weeks may lead to some tolerance to their effects on sleep patterns 3. Anesthesia • some sedative-hypnotics stage III of GA • large doses contribute to post-op resp. depression • no analgesic property, used as adjuncts, “conscious sed.”
Organ Level Effects • Anti-Convulsant Effect - inhibit development and spread of seizure activity in CNS • - benzodiazepines: clonazepam (for absence seizure), lorazepam, diazepam (drug of choice for status epilepticus) • - barbiturates: Phenobarbital, metharbital 2. Muscle Relaxation • inhibitory effects:polysynaptic reflexes/internuncial trans. • relax contracted skel. muscle/muscle spasm: treat spasticity 3. Effects on Respiratory and Cardiovascular Functions • significant resp. depression in pxs with pulmonary disease • significant CV depression in pxs who are hypovolemic, w/ congestive heart failure or w/ impaired CV function
Benzodiazepine Antagonist: Flumazenil • MOA: competitive antagonism at GABAA receptor • 1,4- benzodiazepine (synthetic) derivative • does not antagonize the CNS effects of other sedative-hypnotics, ethanol, opioids or general anesthetics • IV; half-life = 0.7 – 1.3 hrs. due to rapid hepatic clearance • Watch/O for recurrence of benzodiazepine-caused CNS dep. • Adverse Effects: agitation, confusion, dizziness, nausea, abstinence symptoms in dependent patients • Drug Interaction: benzodiazepine + tricyclic antidep. + flumazenil Sz, cardiac arrhythmias
New Anxiolytic • BUSPIRONE: for relief of Anxiety • no marked sedation/euphoria; less psychomotor impair. • does not potentiate CNS actions of other drugs • Mechanism of Action: partial agonist at 5-HT1A receptor • Onset of Action: > one week to establish • Not for panic states, only for general anxiety states • Liver dysfunction may decrease clearance • Drug Interactions: • Buspirone + MAOI BP • antagonized by flumazenil
New Hypnotics • ZOLPIDEM (Stilnox):a hypnotic • Mechanism of Action: binds selectively with BZ1 (omega1) subtype of benzodiazepine receptor • facilitate GABA-mediated neuronal inhibition • antagonized by flumazenil; elim.half-life: 1.5 – 3.5 hrs. • DI: • dose in pxs w/ liver dysfunction, elderly, on cimetidine • Rifampicin (C P450 inducer) half-life of zolpidem • C/I: children <15 yrs., pregnant/lactating pxs • Prep: tab 10mg
New Hypnotics • 2. ZALEPLON: a hypnotic, resembles zolpidem • Mechanism of Action: binds selectively with BZ1 receptor subtype of benzodiazepine receptor • facilitate GABA inhibitory action • decreases sleep latency, has little effect on total sleep time • SE: amnestic effects; next-day impair. of psychomotor fx • may potetiate CNS depression from ethanol • no reports of tolerance or withdrawal symptoms • Pharmacokinetics: • absorbed rapidly from the GIT • metabolized by hep.aldehyde oxidase, cytochrome p450 • metabolism is inhibited by cimetidine
Sedative - Hypnotics • DRUG INTERACTIONS • 1. Additive Effects with Other CNS Depressants • alcoholic beverages, opioidcs, anti-convulsants, phenothiazines, antihistamines, TCAD, antihypertensives • 2. Altered Activity of Hepatic Drug-Metabolizing Enzyme System • Barbiturates - metabolism of dicumarol, phenytoin, digitalis, griseofulvin • Diazepam – half-life doubled by cimetidine (inhib. metab Chloral Hydrate – may displace warfarin from plasma protein binding sites anticoagulant effect of warfarin
Clinical Toxicology of the Sed-Hyps • CNS Depression • - severe toxicity: resp. dep., aspiration, loss of vasomotor control from brainstem, direct myocardial depression • - treatment:secure airway and breathing, maintain plasma volume, renal output,maintain cardiac function, • reversal of benzodiazepine effects by flumazenil 2. Hypersensitivity Reactions – skin rashes 3. Teratogenicity – piperidindiones, some benzodiazepines 4. Enhance Porphyrin Synthesis • - barbiturates are contraindicated in patients with acute intermittent porphyria, variegated porphyria, hereditary coproporphyria or symptomatic porphyria
Alterations in Drug Response • 1. Tolerance - decreased responsiveness to a drug following repeated exposure • depends on dosage, duration of use, chronic abusers consume very large doses w/o experiencing severe toxicity • Cross-Tolerance – exists between different sedative-hypnotics, including ethanol • 2. Physiologic Dependence • altered physiologic state requiring continued drug administration to prevent the appearance of abstinence Sx • withdrawal Sx: restlessness, anxiety, weakness, orthostatic hypotension, hyperactive reflexes, generalized seizures • Cross-Dependence – the ability of a substituted drug to suppress abstinence Sx from D/C of another drug