Download
1 / 25
280 likes | 485 Vues
BIOCHEMİCAL EVALUATION OF ANEMIA. Prof.Dr.Arzu SEVEN. Biochemical evaluation of anemia. Hemolytic disorders resulting from erythrocytic enzyme abnormalities: a)enzymes of Emden-Meyerhof Pathway of anaerobic glycolysis -hexokinase -glucose phosphate isomerase -phosphofructokinase

E N D
BIOCHEMİCAL EVALUATION OF ANEMIA Prof.Dr.Arzu SEVEN
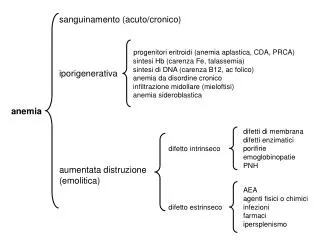
Biochemical evaluation of anemia • Hemolytic disorders resulting from erythrocytic enzyme abnormalities: • a)enzymes of Emden-Meyerhof Pathway of anaerobic glycolysis -hexokinase -glucose phosphate isomerase -phosphofructokinase -triosephosphate isomerase -phosphoglycerate kinase -pyruvate kinase
b)hexose monophosphate pathway -transketolase -glucose 6-phosphate dehydrogenase(G6PD) • c)glutathione pathway -GSH peroxidase -GSH synthetase
d)purine pyrimidine metabolism -adenosine triphosphatase -adenosine deaminase -pyrimidine-5'-nucleotidase
Pyruvate kinase deficiency • Most common • Autosomal recessive • Mild severe • İnability to synthesize ATP for RBC metabolism, ion gradients γ cell shape • 2,3 BPG -O2 affinity -O2 delivery to muscle γ fetus
G6PD deficiency • Genetic • Mutation • Common in Mediterenean γ Africo_Carribbean origins • NADPH • GSH can not be regenerated from GSSG • GSSG , H2O2 , radicals
Oxidative challenge: -oxidants (antimalarial primaquine, aspirin, sulfonamids) -severe infections -fava beans • Primaquine sensitive hemolytic anemia • Peroxidation of lipids in RBC membrane RBC lysis
Iron deficiency anemia • A common nutritional problem seen especially in menstruating γ pregnant women • ♂ 1 mg iron/day • Mensruating ♀ ~ 2mg iron/day • Pregnant ♀ ~3mg iron/day
Megaloblastic anemia • Inadequate folate intake impaired absorption impaired metabolism increased demand (pregnancy, lactation) folate deficiency methionine nucleic acid
Enlarge blast cells in bone marrow • Macrocytic RBC with fragile membranes tendency to hemolyze (macrocytic anemia) • Folate supplementation (400 mg/day) during periconception period (4 weeks before γ 8 weeks after conception) prevents neural tube defects in spina bifida and hyperhomocysteinemia)
Pernicious anemia • PA is a conditioned nutritional deficiency of cobalamin by failure of gastric mucosa to secrete IF • Inadequate intake of vit B12 extremely rare • Defective production of IF most common • Genetically determined, but not manifested until late in life
vit B12 deficiency folate deficiency • IF deficiency in the stomach prevents vit B12 absorption in terminal ileum • gastric surgery surgical removal of ileum IF (Crohn's disease) vegans vit B12
Gastrointestinal symptoms (episodic abdominal pain, constipation γ diarrhea) • Atrophic gastritis • Immune abnormalities: antiparietal cell antibodies anti-IF antibodies
Liver disease associated with alcoholism may lead to folate_deficiency megalosblastic anemia • During the investigation of the cause of megaloblastic anemia, folate must be given together with B12 vit.(to prevent neuropathy)
Correlation of vit.B12 and folate levels with clinical status:three laboratory tests need to separate four clinical situations
Methods for the determination of vitamin B12 and Folic acid • Microbial assay • Competitive protein binding assay • Immunometric assay
Indirect methods for assessment of vitamin B12 deficiency • Methylmalonic acid assay • Measurement of homocysteine • Deoxyuridine suppression test • Vit.B12 absorption (Schilling) test • Tests for intrinsic factor blocking antibodies
Because vit.B12 is needed for the conversion of methylmalonic acid to succinic acid , patients deficient in vit.B12 excrete excess amounts of methylmalonic acid in urine
Homocysteine is increased in the plasma of patients who are deficient in vit.B12 because their cells can not metabolise homocysteine to methionine at a normal rate • The increase in plasma homocysteine may precede the typical signs of macrocytic anemia and decreased cobalamin
Schilling test permits differentiation of causes of vit B12 deficiency (pernicious anemia or intestinal malabsorption)