Download
1 / 48
1.7k likes | 3.99k Vues
PTP 512 Neuroscience in Physical Therapy Postural Control. Reading Assignment Shumway-Cook: pp. 161-162, 164-193 Min H. Huang, PT, PhD, NCS. Objectives. Define postural control and distinguish between postural orientation and stability Describe the concepts of dynamic stability limits

E N D
PTP 512Neuroscience in Physical TherapyPostural Control Reading Assignment Shumway-Cook: pp. 161-162, 164-193 Min H. Huang, PT, PhD, NCS
Objectives • Define postural control and distinguish between postural orientation and stability • Describe the concepts of dynamic stability limits • Describe postural control processes, including the contribution of the motor action component and the role of sensory functions • Compare and contrast feedback vs. feedforward postural control • Discuss the attentional demands of postural control and its impact on stability during multi-tasks
Postural Control Defined • Postural Control • Controlling body position in space for • Stability • Orientation • Postural Orientation • Ability to maintain an appropriate relationship between body segments and between the body and the environment
Base of Support (BOS) • BOS is the area of the body in contact with the support surface
Gait: Chasing COG“Walking is a state of constant falling” • During gait, the COG falls anterior to the BOS and the person must step forward to re-establish the COG within the BOS to avoid falling
Center of Pressure (COP) • COP is the center of the distribution of total forces applied to the support surface • COP represents the average “location” of these forces but NOT the forces! It is a point on a 2-D plane! • CNS activates muscles to change the location of COP, which in turns shifts the location of COG Biodex Balance System
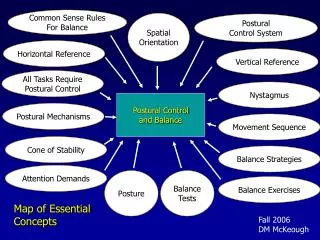
Systems for Postural Control Horak et al., 2009
Postural Stability = Balance • Balance is the ability to keep the vertical projection of the center of mass (COM), within the limits of base of support • COM is a point in 3-dimensional space, usually around L2 in standing • COG is the vertical projection of the COM on a 2-dimensional plane, usually the ground
Stability Limits • Stability limits refer to the boundaries within which the body can maintain stability without changing the base of support. • Previous concepts of stability limits only consider the area of the feet utilized to maintain balance rather static concept Horak et al., 1989 McCollum & Leen, 1989
Current Concepts of Dynamic Stability Limits • Stability limits result from the interaction between the velocity and position of COM. • Stability limits are the boundaries of the combined COM velocity and position possible withoutthe needs to change the base of support • Other factors, such as muscle strength, range of motion, fears of falls, perceived stability, and various aspects of the environment (e.g. lighting, icy vs. dry) also affect the stability limits.
COM displacement-velocity trajectory. Subjects stood on a platform that moved unexpectedly. Left: Stepping response. COP velocity exceed the velocity threshold. Right: Non-stepping response. COM did not cross the stability boundary. Triangle symbol indicates the initial quiet standing position. Pai 2000
Current Concepts of Dynamic Stability Limits: Try this……. • Lean forward as far as possible and then • Throw your arms up as fast as possible • Throw your arms up as slowly as possible • Which condition do you feel more stable? • Stand in your neural upright position • Lean backward as fast and as far as possible • Lean backward as slowly and as far as possible • Which condition do you feel more stable? Which condition are you able to lean further backward?
Modes of Postural Control:Feedback vs. Feedforward Processes Slip on the ice or trip over your cat vs. Any voluntary movements Kandel, 1991
Mode of Postural Control • Feedback control (Compensatory or reactive postural responses) • Sensory feedback from unexpected external perturbations triggers postural responses • Feedforward control (Anticipatory postural control) • Postural responses are made prior to voluntary movement that is potentially destabilizing in order to maintain stability during the movement
Quite Stance Postural Control • Body alignment: ideal alignment requires the least amount of energy • Postural Tone: activity in antigravity postural muscles increases to counteract the gravity • Same muscle synergies used during perturbed stance also play a role in maintaining quiet stance.
Postural Control during Perturbed Stance • Earlier studies of postural control used a platform that moves in the anteroposterior direction. Subjects were asked to keep their feet in place. • These studies found……….. Moving Platform Studies
Movement Strategies to Recover Anteroposterior Stability Ankle Hip Stepping
Ankle Strategy • Distal to proximal muscle activation pattern • Body sways at ankles with hips and knees in relatively extended positions • Utilized in response to small perturbations on firm surface
Hip Strategy • Proximal muscles activated first • Produces large, rapid motion at hip joints • Utilized when standing on narrow BOS (e.g. beam), on soft surface, or during larger, faster perturbations
Stepping or Reaching Strategy • When subjects were not asked to keep feet in place, they more frequently step or reach, instead of utilizing ankle or hip strategies to restore balance (McIlroy & Maki, 1993) • Stepping or reaching are natural responses, not the last resort to restore balance! • Older adults more frequently step than young adults (Mille, 2003) Horak, 2009
Movement Strategies to Recover Mediolateral Stability • Controlled primarily through lateral hip and trunk movement • Proximal to distal muscle activation pattern • Loading and unloading of the two legs controlled by hip abductors & adductors Head motion occurs in the opposite direction of hip and ankle movement Head movement Hip movement (ABD, ADD) Ankle movement
Movement Strategies to Recover Multidirectional Stability There is a continuum response patterns that control stability in the 360-degree of possible perturbation directions Shumway-Cook, 2007
Movement Strategies to Recover Multidirectional Stability • Complex postural response patterns in 360-degree cannot be explained by simple ankle or hip strategies. • Current concepts: • Synergies are flexible. each muscle belongs to more than one synergy • Within each synergy, each muscle has a unique or fixed weighting factor that represents the level of activation of that muscle within the synergy
Each synergy activates a specific set of muscles in a fixed amount. Different combinations of synergies are activated based on continuous sensory feedback to adjust postural stability. Ting, 2005
Clinical Implications of Movement Strategies for Postural Control • Both quiet stance and recovery of stability in response to perturbations use common postural synergies. • Training in one context, e.g. quite stance, may transfer to improve stability in the other context, e.g. recovery of perturbed stance • Do not limit training to the activation of a specific synergy, e.g. ankle or hip strategy
Adapting Strategies • Adaptation is the ability to modify response according to the task demands • With repeated perturbations, movement strategies change (within 5-15 trials!) • Several studies in normal adults found reduced sway with repeated exposure to platform movements
Anticipatory Postural Adjustments (APAs) • Work with a partner. Stand with your arm outstretched, at about waist height, palm up. • Place a heavy book on your outstretch palm. • Have your partner remove the book • Lift the book using your opposite arm • Are the responses different between 1 vs. 2 and why?
Anticipatory Postural Adjustments (APAs) In A, Gastroc was activated prior to biceps. In B, subject was support at the shoulders so the arm movement did not disturb posture. Thus, APAs were not needed. Cordo & Nashner, 1982
Anticipatory Postural Adjustments (APAs) • Postural muscles are activated prior tothe prime movers that produce movement • Same postural synergies utilized during quiet stance and postural perturbations are also utilized in APAs. • In Cordo and Nashner’s study (1982), A & B had different “Central Set”, which refers to the state or readiness of the nervous system that is determined by the context of a task
Clinical Implications • APAs increase with ↑ movement magnitudes and speed. APAs more frequently present with faster movements and heavier loads • Practice can affect the timing of APAs, e.g. dancers activate APAs much earlier in a leg-lifting task than untrained individuals • APAs are reduced when a support is given Your patients will never improve balance if they practice balance tasks while holding on to // bars!
Neural Systems Controlling Postural Orientation and Stability Spinal Cord Brainstem Regulation of postural tone Integration of sensory information Contribute to anticipatory postural control for voluntary movements • Spinal cats can activate extensor muscles to support body but their postural stability is poor • Postural stability is NOT organized at the spinal cord level
Neural Systems Controlling Postural Orientation and Stability • Basal ganglia-cortical loop controls postural set, i.e. the ability to modify the postural muscle activation patterns to changes in the task or environmental conditions Patient with Parkinson’s Disease
Neural Systems Controlling Postural Orientation and Stability • Cerebellar-cortical loop controls the adaptation of postural muscle activation amplitudes, i.e. scaling, in response to changes in task and environmental conditions • Patients with damage to cerebellum were unable to modify postural muscle activation amplitudes even after repetitive perturbations of the support surface (Horak and Diener, 1994).
Sensory Contributions to Balance • CNS processes information from sensory receptors throughout the body to determine the body’s position in space • Vision (especially peripheral vision) • Somatosensation (proprioception, cutaneous, joint receptors) • Vestibular system • Each sense provides a different frame of reference, i.e. “map”
Sensory Weighting Hypothesis • Postural control system is able to reweight sensory inputs in order to optimize stability in altered sensory environments. • The “gain” of a sensory input will depend on its accuracy as a reference for body motion. • Try this. Stand on one leg with eyes open vs. closed. Which sense(s) may be “weighted” when you close your eyes?
Visual Contributions • ↑ sway in young children and old adults with room oscillation (may be due to reduced somatosensation) • Vision may not be reliable • Self motion vs. object motion? Moving Room Experiment Lee and Aronson, 1974
Somatosensory Contributions • Somatosensory contributions typically dominate postural control in response to transient or fast surface perturbations (in this type of situation, visual and vestibular inputs do not help) • Lightly touching a stable surface reduces sway significantly. The somatosensory inputs from the touch, rather than the contact force through touching a surface (Jeka, 1994; Lackner, 1999)
Vestibular Contributions • Typically vestibular system contributes less than somatosensory system • For example, CNS cannot tell whether it is just head bending forward or the whole body is leaning forward • Vestibular system provides a frame of reference relative to the gravity
Testing Adaptation of Postural to Changing Sensory Conditions:Sensory Organization Test (SOT)
SOT Normal Results • Adults and children over age 7 easily maintain balance on all conditions • Least sway on conditions 1, 2, & 3 where the support service is providing accurate sensory information • Greatest sway on conditions 5 & 6 because only one set of sensory inputs (vestibular) are accurate and available • Visual cues are more important when the balance task becomes more challenging
Cognitive Contributions to Balance • Dual-task paradigms • ↓ performance in either task because of limited capacity in information processing to handle both tasks simultaneously • Different postural and secondary tasks affect postural control differently • Older or balance-impaired individuals increase postural sway with ↑ difficulty of secondary cognitive tasks
Cognitive Contributions to Balance • As the difficulty for maintaining stability ↑ , there is ↑ in attention resources required by the postural control system • What type of secondary cognitive task will affect balance is still unclear • Executive function may be the most important cognitive function required to maintain normal balance under dual-task paradigms
Testing Executive Function during Walking: Walking Trail Making Test (W-TMT) Wright, 2011
Balance-impaired older adults with depression required ↑time to step accurately under cognitively challenging conditions that require executive function. MDD: Major depressive disorder ND: Non-depressed * Wright, 2011