Download
1 / 4
240 likes | 2.14k Vues
NOACs vs. warfarin: Pros and Cons for Patients and Providers to Consider. Disadvantages of NOACs Higher out-of-pocket costs and copays No clear advantage over well-controlled warfarin BID dosing may have negative impact on compliance

E N D
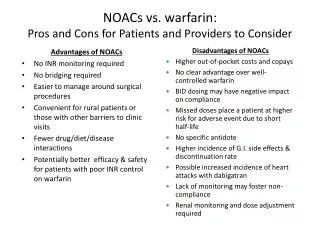
NOACs vs. warfarin: Pros and Cons for Patients and Providers to Consider Disadvantages of NOACs • Higher out-of-pocket costs and copays • No clear advantage over well-controlled warfarin • BID dosing may have negative impact on compliance • Missed doses place a patient at higher risk for adverse event due to short half-life • No specific antidote • Higher incidence of G.I. side effects & discontinuation rate • Possible increased incidence of heart attacks with dabigatran • Lack of monitoring may foster non-compliance • Renal monitoring and dose adjustment required Advantages of NOACs • No INR monitoring required • No bridging required • Easier to manage around surgical procedures • Convenient for rural patients or those with other barriers to clinic visits • Fewer drug/diet/disease interactions • Potentially better efficacy & safety for patients with poor INR control on warfarin
Dabigatran and RivaroxabanFormulary Recommendations:Inpatient • Add to UNMH inpatient formulary only for the purpose of continuing the drug in patients on dabigatran prior to admission that have been deemed to be good candidates for the drug • No initiation of dabigatran in-house • If a patient with new onset non-valvular afib needs anticoagulation, warfarin should be initiated • If a provider wishes to ultimately switch the patient to dabigatran for valid reasons (see outpatient criteria), this should be done in the outpatient setting • Other uses of dabigatran will be reviewed as a nonformulary medication on a case-by-case basis
Dabigatran and RivaroxabanFormulary Recommendations:Outpatient • Add to UNMH outpatient formulary for patients with non-valvular atrial fibrillation and at least one of the following: • history of poor INR control on warfarin despite good compliance • considerable barriers to routine monitoring, such as physical or transportation issues • documented warfarin allergy • documented history of non-hemorrhagic adverse effects with warfarin • documented, confirmed warfarin failure such as an ischemic stroke while consistently therapeutic on warfarin • Reason for using dabigatran instead of warfarin should be clearly documented in the medical record by the prescriber prior to initiation of dabigatran therapy. • Approval for dispensing dabigatran will need to be obtained from the Director of Clinical Pharmacy or their designee for UNM Care patients OR prior authorized by Molina Medical Director for SCI patients.
Dabigatran and RivaroxabanFormulary Recommendations • In all cases where dabigatran will be prescribed, providers will be responsible for ensuring insurance coverage, obtaining prior authorization, if required, and determining patients ability to obtain dabigatran prior to prescribing. • Any prior authorization or approval need to be documented in the patient’s medical record.