Download
1 / 24
240 likes | 405 Vues
Breathing Mapping. The Mapping Process (Mark). Cut & paste into spreadsheet Breathing statements in 6 domains Resus and stabilisation Investigation, data interpretation, diagnosis Organ system support and related practical procedures Monitoring and clinical measurement Use of equipment

E N D
The Mapping Process (Mark) Cut & paste into spreadsheet Breathing statements in 6 domains Resus and stabilisation Investigation, data interpretation, diagnosis Organ system support and related practical procedures Monitoring and clinical measurement Use of equipment Specific circumstances General Paediatric Care of the newborn Peri-operative Care Trauma and burns Transport Pre- and Post-ICU care 4 elements Knowledge Skills Attitude & behaviour Workplace training objectives
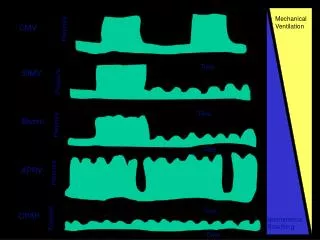
The Mapping Process • Each statement assigned to one of 7 phases in the intubation process • Communication, leadership and teamwork • Assessment of patient • BMV LMA • Intubation • Equipment • Drugs • Failed intubation
The Mapping Process • Each statement assigned to one of 7 phases in the intubation process • Communication, leadership, teamwork , attitudes, safety • Assessment of patient • Specific pathology • Practical diagnostic / therapeutic skills • Equipment • Ventilation (general) • Ventilation (specific circumstances) • Drugs • Complications
The Mapping Process: Themes Communication, leadership and teamwork • Take control • Physiological safety first – including equipment and monitoring • Knowledge of limitations - Get senior help where appropriate • Consideration of ethical issues and appropriate ICU admission • Communication with other teams including laboratory to make diagnosis and establish care plan • Clear explanations / reassurance to other staff, patient, family • Rapid response and resuscitation ‘golden hour’ • Difference between support and treatment • Insist on stability before transfer
The Mapping Process: Themes Assessment of the patient • Clinical features of respiratory compromise • Diagnose and quantify disease severity • Knowledge of early warning / trigger scores • Accurate history including co-morbidities • Accurate clinical exam • Recognize congenital abnormalities • Info from notes, ICU or ward chart • Limited + expanded differential • Integrated management plan (co-morbidities + acute presentation)M • Risk factors for re-admission to ICU following discharge • Plan for rehabilitation
The Mapping Process: Themes Specific Pathology • Common emergencies (asthma, respiratory failure) • Common acute resp pathology (pneumonia, collapse/consolidation, pulmonary oedema, ALI, ARDS, pleural effusion, UAO, LAO) • Prevention and management of pulmonary aspiration • Detection and management pneumothorax • Neonates (RDS, CLD, Preterm baby, congenital abnormalities, antenatal influences) • Trauma (abdo + thoracic, smoke inhalation, fat embolism) • Post-op (thoracotomy, cardiac, lung resection) • Pulmonary hypertension, pulmonary embolism • Acute + chronic disease • Air transport
The Mapping Process: Themes Practical diagnostic and therapeutic skills • Blood gas • Respiratory function tests, • Pulse oximetry and capnography • Inspired and expired gas monitoring • CXR • Microbiology • Bronchoscopy indication + method – intubated / awake • Monitoring devices (principles, indications, contraindications, interpretation, source of error, complications) • ICD insertion • Surfactant administration • BAL • Manual bagging and tracheal suction • Resolve contradictions between clinical info and monitor • Avoidance of unnecessary tests
The Mapping Process: Themes Use of Equipment • Indications for and methods of ventilatory support • Knowledge of ventilator + ventilatory modes • Non-invasive ventilation • Principles of ECMO • Long term / home ventilation • Anaesthesia (Check ventilator, breathing system, monitoring , storage and safe use of gases) • Setting up and checking the ventilator (trouble shoot mis-assembly) • Institution and maintenance of ventilation • Specific circumstances: ARDS, post-op admission, preterm baby • Ventilator alarms • Principles of weaning • Safe extubation • Shared responsibility for equipment with nursing and technical staff
The Mapping Process: Themes Drugs • Pharmacology of hypnotics, analgesia and relaxants • Side effects of drugs and their interactions • Antibiotics – appropriate prescribing, colonization vs infection • Guidelines for surfactant administration
The Mapping Process: Themes Complications • Aspiration • Secondary infection • Detection and management of complications of ventilation • Management and avoidance of cardiovascular and respiratory changes during and after intubation
Scenario Library • Management of the preterm baby • ARDS • Asthma • Child with CLD and pneumonia • Newly diagnosed cardiac - respiratory presentation requiring intubation ? CCF ? Intercurrent resp illness • Take back from Cardiac OT • Management of deteriorating ventilated patient • Bronchiolitis requiring ECMO / ECMO referral • Thoracic trauma • Burns /Smoke inhalation • Failed extubation
Scenario : Management of the Preterm baby • Call to A&E • Unexpected delivery of preterm infant • Establish history from staff + patient / partner • Prepare resuscitaire and equipment • Call for appropriate help • Intubation and delivery of surfactant • Establish ventilation • Identification of any other congenital abnormalities ?CCAM / CDH • Further resus / management as appropriate • Liaison with neonatology team • Preparation for or safe transfer of baby
Scenario : Asthma • 10 year old 60 kg • PMH brittle asthma, frequent short course steroids, short stature • Admitted with 2 week history of URTI and sudden onset severe DOB & wheeze at school today • Capillary gas pH 7.3, CO2 6.9 • Outreach call • Give appropriate advice • Review on ward – assess as exhausted • Arterial gas pH 7.23, CO2 10, pO2 8.9 in 15l non-rebreathe • Intubate with appropriate preparation – consider drugs + team preparation of disaster scenario • Establish ventilation • Use of flow loops, iPEEP etc
Scenario : ARDS • Patient admitted from OT following laparotomy for rupture appendix • Aspirated at induction • Volume requirement 50 ml/kg intra-operatively • Difficult to ventilate at end of case • Handover from surgical team + anaesthetist • Clinical examination • Consideration of appropriate diagnoses and investigations e.g. CXR • CXR:ARDS • Adjust ventilator appropriately • Consider adjuvant strategies (muscle relaxation, fluid requirement antibiotics etc)
Scenario : Child with CLD + pneumonia • History from family • Assessment of patient + relevant investigations (gas / CXR) • Establish NIPPV • Consider previous micro and appropriate choice antibiotics • Discussion re appropriateness of ventilation • Deterioration • Intubation • Aspiration event • Management post intubation
Scenario : Pulmonary oedema • Call to Paed assessment unit • 4 month old with severe respiratory distress • O/E Blue, Pansystolic murmur and wide spread creps • Requires urgent intubation • Establish ventilation • Ix as appropriate. Treatment strategy • ECHO – VSD • Revise treatment plan • Phase 2 – ventilated x 8 days: assess for extubation • Phase 3 - Failed extubation – consider UAO, malacia, if post-op the diaphragm as well
Scenario : Take back from OT: Cardiac • Preparation for patient including ventilator set up • Handover process • Child has open chest • Establish ventilation and monitoring • Choice of mode and setting of parameters and alarms • Set alarms • Consideration of cardio-resp interactions • Blood gas interpretation • Interpretation of flow loops • Ventilator malfunction – trouble shooting
Scenario : Management of ventilated patient • Called to assess patient with increased CO2 on gas • Blood gas interpretation – review of bedside chart • History from staff at bedside secretions etc • Clinical examination • Consideration of appropriate diagnoses and investigations e.g. CXR • Manual bagging and suction • BAL • Bronchoscopy for reinflation of collapsed lung • Use of DNAase • Recruitment • OR • Pneumothorax • Chest drain insertion
Scenario : Bronchiolitis requiring ECMO • 4 month old ventilated for RSV + bronchiolitis • Called by SHO to review as gases deteriorating • Assessment and optimisation of management • Discussion with consultant re ECMO • Referral for ECMO or activation of ECMO team • Preparation for ECMO
Scenario : Thoracic trauma • Call to A&E • 8 month old, no history of trauma • Severe respiratory compromise • O/E Extensive subcut emphysema • CXR • Bilateral pneumothoraces and rib fractures • Intubation and chest drain insertion • Secondary survey • NAI
Scenario : Burns / Smoke inhalation • 8 year old discharged to HDU from ICU this am following ventilation for smoke inhalation (house fire) • Increased work of breathing and confusion over course of evening • BiPAP commenced • Child has had large vomit and acutely deteriorated • Urgent intubation • CXR – new changes consistent with aspiration • Establish ventilation • Consideration of other diagnoses for confusion – CO, head injury etc
Scenario : Failed extubation • Tag on weaning plan, assessment for extubation, failed extubation to any scenario