Download
1 / 14
160 likes | 1.39k Vues
Case report of a Modified Radical Mastectomy performed under Thoracic Epidural Anesthesia. Dr Lukram Ajit Singh MBBS, DNB (Gen Surgery). Sr Registrar Oncosurgery Dr Gautam Mukhopadhyay Consultant Oncosurgeon & HOD of Onco surgery Dr Abhijeet Banerjee Anesthetist. Case history in brief:.

E N D
Case report of a Modified Radical Mastectomy performed under Thoracic Epidural Anesthesia Dr Lukram Ajit Singh MBBS, DNB (Gen Surgery). Sr Registrar Oncosurgery Dr Gautam Mukhopadhyay Consultant Oncosurgeon & HOD of Onco surgery Dr Abhijeet Banerjee Anesthetist
Case history in brief: • Mrs. SB Ray a 70 years old lady and a resident of Barrack pore presented with a breast lump in her right breast on 11/08/10. The lump was there for 2 months, gradually increasing in size. • On clinical evaluation, there was a hard lump with irregular surface and borders measuring 4/4 cm in size and occupying the upper outer quadrant of the right breast. The lump was not fixed to skin and surrounding tissues. • No axillary nodes were palpable and no signs of distant metastasis was present. • FNAC: Duct carcinoma of right breast.
Staging and Plan • Stage: Clinical staging T2 N0 M0 • Plan : Modified Radical Mastectomy Co morbidities in the patient prevented us from going ahead with a routine MRM. On further work up for surgery patient was found to have a very poor pulmonary function test and was declared unfit for general anesthesia by the medical team (anesthetist, chest and general physicians) looking after her.
Dilemma • An operable case of breast cancer and the brave 70yrs old lady ever willing to undergo any type of surgery to make her life cancer free and the poor lung compliance made us think out of the box. • We planned to go ahead with the MRM under thoracic epidural anesthesia and try our best to treat this lady.
Informed consent and surgery • After discussion about the technique and nature of the procedure with the patient and her relatives, we went ahead with our planned MRM under thoracic epidural anesthesia on 14/08/2010. • Patient underwent modified radical mastectomy with complete axillary clearance upto level III. • The procedure was uneventful, surgery was satisfactory and the thoracic epidural anesthesia that we chose worked well !!
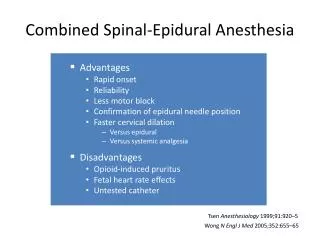
Thoracic epidural anesthesia • Is a safe way of anesthesia in patients unfit for GA. • Our surgery is one of the rare recorded MRM s performed under thoracic epidural anesthesia. • Patient was given her due treatment through this form of anesthesia. • She had come back after the surgery for follow up and received her 1st cycle of chemotherapy.
My first 2 weeks in the dept of Oncosurgery at Ruby General Hospital • This is my log book in 14 days(Sept1 to 14) and is still counting: Total =21 cases • Modified Radical Mastectomy- 5 cases • Hemimandibulectomy-3 cases • Oral Laser surgery- 4 cases • Total Thyroidectomy- 2 cases • Modified Radical Neck Dissections- 3 cases • Abdomino perineal resections- 1 case • Exploratory laparotomy and enterostomies-2 • Excision of soft tissue malignancy-1
DECOMPRESSION ENTEROSTOMY-PALLIATIVE SURGERY IN INOPERABLE GI CANCER