Download
1 / 49
500 likes | 818 Vues
Latent Tuberculosis Infection (LTBI) Case Study. Learning Objectives (a). After completing the case study, the learner will be able to: Name at least 3 groups at high risk for developing tuberculosis (TB) once they are infected with M. tuberculosis

E N D
Learning Objectives (a) After completing the case study, the learner will be able to: • Name at least 3 groups at high risk for developing tuberculosis (TB) once they are infected with M. tuberculosis • Describe how to properly measure and record a tuberculin skin test (TST) reaction
Learning Objectives (b) • Describe the situations in which a TST reaction is interpreted as positive or negative, including when there’s a history of BCG vaccination • Describe the appropriate follow-up for “positive TST” contacts • Explain how to evaluate a patient with a positive TST for active TB
Learning Objectives (c) • List options for treating LTBI • Name at least 3 symptoms to monitor in patients being treated for LTBI
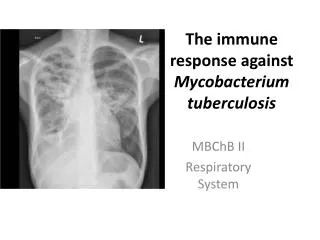
Part 1 (a) • Lenore Davis, 26, hospitalized for cough, fevers, night sweats and weight loss over several months • TST = 19mm • Chest radiograph revealed a right mid-lung airspace opacity
Part 1 (b) • Lenore is HIV-negative • Smear- and culture (+) for M. tuberculosis, with drug susceptibility results pending
Part 1 (c) Home contacts: • Mary, 52, Lenore’s mother who owns the home in which they live. Currently taking 20 mg of prednisone a day to treat her rheumatoid arthritis
Part 1 (d) • Rhonda, 31, Lenore’s sister who struggles with unemployment and mental health problems; periodically stays with Lenore and her mother; HIV(+) • Lucy, 2, Rhonda’s daughter who lives full-time with grandmother, Mary, who has legal custody of her
Part 1 (e) Work contacts: • For the past year Lenore has been working at a series of temporary clerical jobs at offices in two neighboring towns • Prior to working as an office temp, Lenore spent 18 months in Southeast Asia, traveling and teaching English
Part 1 (f) Social contacts: • Fernando, 27, Lenore’s boyfriend, Filipino immigrant (8 yrs in U.S.); sees Lenore daily • Esperanza, 50, Fernando’s mother; Lenore and Fernando visit her home 3 times/week. Esperanza is Filipino immigrant (8 years in U.S.) and healthcare worker
Part 1 (g) • Colleen, 26, Lenore’s best friend; spends most weekends with Lenore shopping at a local mall • Larry, Francie and Pete, former college friends who Lenore meets monthly in a local park to play softball
Question 1 How do you proceed?
Answer Choices (a) • Ask Lenore when her TB symptoms began to determine her period of infectiousness • Order TST and symptom review for: • Mary (mother, RA) • Rhonda (sister, HIV+) • Lucy (2-year-old niece)
Answer Choices (b) • Order TST and symptom review for (continued): • Larry, Francie and Pete (softball friends) and any others who joined in the monthly softball games in the last few months • Fernando (boyfriend) • Esperanza (boyfriend’s mother)
Answer Choices (c) • Order TST and symptom review for (continued): • All staff and clients at offices where Lenore worked for last few months • Colleen (best friend) • Clerks at all stores where Lenore and Colleen shopped in last few months
Answer Choices (d) • Offer HIV counseling and testing for all close contacts whose HIV status is not known
Part 2 (a) • Lenore’s cough began around Thanksgiving (two months ago) • You assess that the following “close contacts” should be screened: • Mary (mother, RA) • Rhonda (sister, HIV+) • Lucy (2-year-old niece)
Part 2 (b) • Fernando (boyfriend) • Esperanza (boyfriend’s mother) • Colleen (best friend) • Coworkers that shared office space with Colleen during the past four months
Question 2 How do you proceed?
Answer Choices (a) • Ask close contacts if they are experiencing any weight loss, coughing, night sweats, or fevers. • Administer TST by tine (multiple puncture) test. • Read TST reactions 48-72 hours after TST is administered.
Answer Choices (b) • Measure the redness (erythema) of the TST reactions. • Record the TST reactions in millimeters, instead of simply as “positive” or “negative.”
Part 3 (a) Results of TST and symptom reviews: • Mary (mother, RA): 0mm, no symptoms • Rhonda (sister, HIV+): 0mm, no symptoms • Lucy (2-year-old niece): 7mm, no symptoms
Part 3 (b) • Fernando (boyfriend): 13mm, no symptoms. Fernando attributes his reaction to BCG vaccinations he received as a child in the Philippines) • Esperanza (boyfriend’s mother): 19mm, no symptoms. Esperanza reports that she “took 3 months of pills and shots” for active TB eight years ago in the Philippines, shortly before immigrating to the U.S.
Part 3 (c) • Colleen (best friend): 15mm, no symptoms. Colleen had a 0mm TST result 6 months ago • Staff that shared office space with Colleen for last 4 months: all < 5mm, no symptoms • All close contacts whose HIV status was unknown have been confirmed as HIV negative.
Question 3 How do you proceed?
Answer Choices (a) • Disregard 13mm reaction of Fernando (boyfriend) due to BCG history • Consider 7mm reaction of Lucy (2-year-old niece) as TST (+); order chest radiograph to rule out active TB. • Consider 15 mm reaction of Colleen (best friend) as TST (+); order chest radiograph to rule out active TB.
Answer Choices (b) • Do not consider Mary (mother, RA) for LTBI treatment because her TST result was 0mm. • Order chest radiograph for Esperanza (boyfriend’s mother) to compare with her baseline chest radiograph on file at the hospital where she works.
Part 4 (a) • Chest radiographs for Fernando (boyfriend), Lucy (2-year-old niece), Colleen (best friend), Mary (mother, RA) and Rhonda (sister, HIV+) are normal. • Comparison of former and recent chest radiographs for Esperanza (boyfriend’s mother, previous TB) shows stable fibrotic lesion; 3 sputum smears and cultures are (-).
Part 4 (b) • Fernando (boyfriend) and Esperanza (boyfriend’s mother, previous TB) agree to begin treatment for LTBI. Fernando describes himself as a “moderate” drinker, consuming 2-3 beers per day. Esperanza says she does not drink alcohol.
Part 4 (c) • When you advise Colleen to begin LTBI treatment, she resists, saying she has only been “exposed” to Lenore’s TB and has no symptoms of the disease. “Why should I take that medicine for so long when I feel fine?” she asks.
Part 4 (d) • Rhonda (sister, HIV+) agrees to LTBI treatment for herself but says she plans to leave the U.S. in a few months to live with a friend in Canada. Rhonda isn’t sure she’ll be able to finish her LTBI regimen; sometimes she forgets to take, or loses, the antiretroviral medication prescribed for her HIV infection.
Part 4 (f) • Mary (mother of Lenore, RA) agrees to LTBI treatment for herself and for her granddaughter Lucy (2 years old).
Question 4 How do you proceed?
Answer Choices (a) • Order baseline liver function tests (LFTs) for all patients being treated for LTBI. • Do not prescribe LTBI treatment for Colleen (best friend, 15mm) because she insists she “feels fine.” • Prescribe a 9-month regimen of INH for Mary (mother, RA).
Answer Choices (b) • Prescribe a 9-month regimen of isoniazid (INH) for Fernando (boyfriend), with pyridoxine (B6) because of his alcohol use. • Prescribe 3 months of INH for Lucy (2-year-old niece). • Prescribe 2 months of rifabutin and pyrazinimide for Rhonda (sister, HIV+).
Answer Choices (c) • Prescribe 4 months of daily rifampin for Esperanza (boyfriend’s mother, class 4). • Dispense medications in 6-month supplies to Fernando (boyfriend), Mary (mother) and Colleen (best friend). • Order medication for Rhonda (sister, HIV+) to be administered via DOT (directly observed therapy).
Answer Choices (d) • Continue to monitor Rhonda (sister, HIV+) at 2, 4, and 6 weeks of treatment • Advise Fernando, Colleen, Rhonda, Mary, and Esperanza to immediately report nausea, loss of appetite, malaise, or rash. • Assume Fernando (boyfriend) will stop his alcohol consumption during treatment as he is advised to do.
Part 5 (a) • Fernando (boyfriend), Mary (mother, RA) and Colleen (best friend) are prescribed 9-month regimens of daily INH to be dispensed at the clinic at one-month intervals. Fernando also receives pyridoxine (B6). • Rhonda (sister, HIV+) is prescribed a 2-month regimen of rifabutin and pyrazinamide to be delivered via DOT.
Part 5 (b) • Lucy (2-year-old niece) is prescribed a 9-month regimen of INH to be administered twice-weekly via DOT. • Esperanza (boyfriend’s mother, class 4) is prescribed a 4-month regimen of rifampin.
Part 5 (c) • 12 weeks after 1st TST, results of 2nd TST for Mary (mother, RA), Rhonda (sister, HIV+) and co-workers are: • Mary: still 0mm • Rhonda: still 0mm • Co-workers: all still < 5mm
Part 5 (d) • The drug-susceptibility results for Lenore (index case) find that her isolate of M. tb is susceptible to all four first-line agents. • As his 3rd month of treatment begins, Fernando (boyfriend) fails to report to clinic for monthly monitoring and to pick up his 30-day supply of INH; Fernando says he’s tired of taking the medicine, and it makes him nauseous.
Question 5 How do you proceed?
Answer Choices • Temporarily suspend Fernando’s regimen; order liver function tests. • Discontinue LTBI treatment for Mary (mother, RA) and Rhonda (sister, HIV+) because their second TST results, after the “window period” has passed, are still 0mm.
Epilog (a) • Fernando’s LFTs were within normal range. You change Fernando’s INH from daily to twice-weekly delivered via DOT. • Mary and Rhonda continue their LTBI treatment regimens.
Epilog (b) • Should the health department close or expand its contact investigation? When there is evidence of recent transmission of M. tb among the first group of close contacts tested, it is more likely that transmission has occurred in other-than-close contacts.
Epilog (c) • In Lenore’s case, two TST conversions occurred: Lucy, age 2, and best friend Colleen, who converted from 0mm to 15mm in the last six months. This evidence supports the decision to expand the contact investigation for Lenore Davis.
Review Questions (a) • Name 3 groups at high risk for developing tuberculosis (TB) once they are infected with M. tuberculosis. • What is the proper method for placing a tuberculin skin test (TST)? How should the reaction be measured and recorded?
Review Questions (b) • Under what circumstances is a TST reaction of > 5mm interpreted as positive? How does a history of BCG vaccination affect the interpretation of the TST reaction? • How should a patient with a positive TST be evaluated for active TB?
Review Questions (c) • What are two options for treating LTBI? • Name 3 symptoms to monitor in patients being treated for LTBI.