Download
1 / 56
560 likes | 736 Vues
Management of Stage 3 Chronic Kidney Disease (CKD) in General Practice Dr. Valli Manickam Renal Physician. Objectives: Statistical data about CKD Target values in ESKD When to Refer patients . 1000. Steady state . Linear growth . 900.

E N D
Management of Stage 3 Chronic Kidney Disease (CKD) in General Practice Dr. Valli Manickam Renal Physician
Objectives: • Statistical data about CKD • Target values in ESKD • When to Refer patients
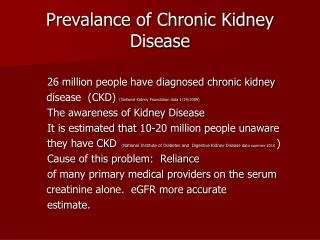
1000 Steady state Linear growth 900 800 ESKD services ($millions) 700 600 500 400 2004 5 6 7 8 9 2010 559.9 640.1 688.0 724.5 754.5 782.3 811.3 Steady state 559.9 652.5 712.9 763.8 808.6 852.5 899.1 Linear growth Why worry about CKD & ESKD? Projected annual ESKD costs Cass et al Kidney Health Australia Report 2006
ESKD has a life expectancy between that of Colon Cancer & Lung Cancer USRDS 2001
ESKD and Cardiovascular Mortality Foley et al AJKD 1996
30 Early Referral 25 Residual Renal Function 20 CreatinineClearance(ml/min) 15 10 5 Late Referral 0 Timely Start ? Why be interested? – Slowing progression
CKD Definitions Adapted from Am J Kidney Dis 2002; 39 (2, Suppl. 1): S17-S31 and using AusDiab data
Stage 5 – kidney failure 16,000 Stage 4 – GFR <30 30,000 Stage 1-3 1.7 MILLION Hypertension or diabetes 4.5+ MILLION AT RISK Kidney Disease in Australia The titanic/iceberg model Adults over 25 years of age AusDiab data, 2005
CKD and the risk of death,CV events and hospitalisation All cause mortality Cardiovascular mortality N = 1,120,295 Go et al N Engl J Med 2004; 351:1296-1305 Kaiser Permanente Renal Registry
Outcomes in patients with CKDKaiser Permanente Longitudinal Study n = 27988, FU = 66 mo Patients with CKD are 20 times more likely to die from cardiovascular events than survive to reach dialysis Keith et al Arch Int Med 2004
Estimated GFR (MDRD)Median and interquartile range GFR and Ageing Prevalence of eGFR < 60 ml/min in popn GFR declines by 5-8mL/min/1.73m2 each decade NHANES III
With CKD Bruce the Battler
Mr Bruce Battamsseen 02/08 74 yo, retired Smoker – 20 / day, alcohol - 30 g/day Hypertension – 20 years DM2 – 5 years Oral hypoglycaemics Diverticular disease Infra-renal AAA – 4 cm Incidental finding on CT for abdo pain Stress echo - no inducible ischaemia Medications: amlodipine, pravastatin, gliclazide, aspirin (low-dose) Bruce the Battler
BP 190 / 84 mmHg Peripheral pulses present Murmur Aortic Sclerosis eGFR mL/min/1.73m2 Creatinine 160 umol/L 37[on 02/08] 115 umol/L 57 [on 09/07] Chol - 6.7 mmol/L: TG - 4.05 mmol/L FBC normal UA trace protein, no RBC, no WBC Bruce the Battler
The absence of significant proteinuria makes diabetic kidney disease extremely unlikely Quantitation of proteinuria will give important prognostic information He should not be started on an RAS inhibitor* to slow progression of kidney disease as he has worsening kidney function His smoking will worsen his kidney function Lipid lowering therapy has been proven to slow progression of kidney disease Question 1: Answer True or False *ACE/ARB
The absence of significant proteinuria makes diabetic kidney disease extremely unlikely FALSE 20-30% of diabetic patients may have chronic kidney disease without evidence of proteinuria Mechanism not well understood Likely to progress with time Question 1 Minerva Endocrinol. 2005 Sep;30(3):161-77
Quantitation of proteinuria will give important prognostic information TRUE Increasing degrees of proteinuria lead to increasing risk of ESKD Proteinuria a stronger marker of risk of progression to ESRD than baseline GFR But eGFR strong predictor of morbidity and mortality Reduction of proteinuria in proteinuric disease predicts reduced mortality and reduced progression to ESKD Question 1
Risk of ESKD related tobaseline proteinuria (dipstick) over 18 year period N= 106,000 Iseki et al, Kidney Int 2003;63:1468-1476
Macroalbuminuria is a better marker than GFR in predicting loss of kidneyfunction N=8952 – F/U 4yrs Reduced GFR – mean 45 mL/min/1.73m2 General Population + RBC urine Macroalbuminuria PREVEND Study J Am Soc Nephrol 2006; 17:2582–2590.
Recommended Targets in CKD Proteinuria and ESRD: • 20-30% of diabetic patients may have chronic kidney disease without evidence of proteinuria • Mechanism not well understood • Likely to progress with time Minerva Endocrinol. 2005 Sep;30(3):161-77
Increasing degrees of proteinuria lead to increasing risk of ESKD • Proteinuria a stronger marker of risk of progression to ESRD than baseline GFR • But eGFR strong predictor of morbidity and mortality • Reduction of proteinuria predicts reduced mortality and reduced progression to ESKD
Albuminuria and GFR predict mortality and morbidity (RR) PREVEND Study J Am Soc Nephrol 2006;17: 2582–2590.
He should not be started on an RAS inhibitor to slow progression of kidney disease as he has worsening kidney function FALSE RAS inhibitors beneficial in decreasing mortality in those with GFR < 60 mL/min RAS preferred agent for BP control in CKD, particularly in those with significant proteinuria Question 1
Risk Stratification - BP 10 mmHg SBP results in 10.9% increase in RR of ESRD(RENAAL STUDY) SBP = PP < DBP in prediction of ESRD PP > SBP > DBP in prediction of mortality PP > 70 mmHg risk mortality in SHEP, FHS
RAS inhibitors beneficial in decreasing mortality in those with GFR < 60 mL/min • RAS preferred agent for BP control in CKD, particularly in those with significant proteinuria
ACEi / ARB independent effect over BP alone Multiple trials DM CTS – ACEi RENAAL – ATII IDNT – ATII Non-DM GISEN REIN Treatment of BP in CKD - ? which agent Bakris Et al AJKD 2000;36:646-661
Question 1 • Smoking is associated with kidney damage in thepopulation AusDiab Study • Smoking increases proteinuria and accelerates lossof GFR Am J Med Sci 2005;330:111-119
Lipid lowering therapy has been proven to slow progression of kidney function FALSE Question 1
No specific randomised trials Post hoc analysis of CVD trials CARE Pravastatin vs placebo Fall in GFR 0.6 mL/min/1.73m2/yr if GFR < 50 mL/min 2.7 mL/min/1.73m2/yr if GFR < 40 mL/min greater effect with increasing proteinuria HPS 40 mg simvastatin vs placebo attenuation in rise of serum creatinine GREACE atorvastatin vs placebo Atorvastatin increased CrCl 12% placebo decrease in CrCl 5 % Does treating lipids affect CKD progression? No trials in GFR <40mL/min/1.73m2
Pravastatin reduces Absolute RR for CV events in DM & CKD – similar benefit seen in all-cause mortality Median F/U 64m Tonelli et al JASN 2005;16:3748
Bruce the Battler Commenced on perindopril/indapamide Seen 2 weeks later and reassessed: BP 150 / 76 mmHg Creatinine 189 umol/L (eGFR : 30 mL/min/1.73m2) – Previously Creat 160 umol/L and GFR 37 mls/mt in Feb 2008. K 5.8 mmo/L Urine ACR 9 mg/mmol
Do you : Cease the ACEi and commence another drug Cease the ACEi and check for a renal artery stenosis Continue the ACEi and check for a renal artery stenosis Add another drug for better BP control Question 2
My answer: Rationale: A rise in creatinine of <30% is not unexpected after BP lowering and is a result of decreased perfusion Target BP in CKD is <130/80 mmHg ACEi may have particular benefit for kidney disease K+ needs watching but not a concern at this level(? Give low K+ diet) Add another drug for better blood pressure control
Bruce the Battler Seen 1 month later BP 134 / 68 mmHg Creatinine 245 umol/L eGFR 23 mL/min Ca 2.05 mmol/L PO41.54 mmol/L Hb 98 g/L normocytic/normochromic Urine dipstick normal
What would you do? Refer for erythropoietin treatment Check iron studies Check Vit B12 and folate levels Check Vitamin D and PTH All of the above Question 3
Bruce the Battler My Answer: e. All of the above Results: Ferritin 996 Tsat 55% B12 and folate Normal TSH Normal PTH 18 pmol/L (N <8 pmol/L) Vit D 25 nmo/L (mod deficiency)
CKD progression - Anaemia • Anaemia due to CKD begins at GFR < 60 mL/min • common when GFR < 30 mL/min (30-40%) • CKD anaemia is a diagnosis of exclusion • Need to ensure not Fe deficient or B12/folate deficient, or hypothyroid • Different reference range for Fe stores if on Erythropoietin • Ferritin > 300 ng/ml Tsat >20% • May respond to iv iron if stores low without need for erythropoietin • I.v. iron gives quicker and higher response than oral (and is better tolerated) Gouva et al, Kidney Int 2004;66:753-760
Anaemia is associated with mortality in dialysis patients Multiple observational studiesshow lower Hb associated with adverse outcome Adjusted RR of death due to any cardiac cause, according to Hct. n= 50,579 Li & Collins, Kidney International 2004;65:626–633
The target Hb for anaemia in CKD • Optimal Hb level not known • Observational – 110 – 120 g/L • RCT – no benefit above 120 g/L
CKD & Anaemia Summary Common and important to correct Can’t start EPO till Hb <100g/L (PBS) Need to have nephrologist endorsement to start Ensure not iron deficient All respond – need to dose titrate Most self administer SC each 2-4wks All will need extra iron (oral or i.v.)
Bruce the Battler Seen 1 month later BP 134 / 68 mmHg Creatinine 245 umol/l eGFR 23 mL/min Ca 2.05 mmol/L PO41.54 mmol/L Hb 98 g/L normocytic/normochromic Urine dipstick normal
Why worry about Ca & PO4in CKD Stages 3-5? • All patients develop Ca/PO4 disturbance (by CKD Stage 5) • Onset of Ca changes is early in CKD Ca/PO4 disturbance causes • Bone disease • Soft tissue calcification (coronaries & valves) • Pruritus • Proximal myopathy • Premature death
Increased PO4 is associated with increased mortality even in normal Kidney Function Hazard ratio S. PO4 mg/dL Tonelli et al, Circulation 2006
Mechanisms of Ca/PO4 disturbance Phosphate retention with reduced GFR results in increased s PO4 and suppresses Vit D3 production Reduced Vit D3 leads to reduced Ca absorption and this plus high s PO4 leads to low s Ca Ca x PO4 increases favouring tissue deposition PTH stimulated by low Ca, high PO4 & low Vit D3 Clinical effects: Low s Ca High s PO4 High s PTH Low Vit D3 [1,25 (OH)2D3 = calcitriol]
Changes Ca/PO4 parameters with reducing GFR Changes in serum levels CKD Stage GFR (mL/min/1.73m2) 1,25D Phosphate Calcium PTH 60-90 2-fold 2 3 30-59 2-fold 15-30 4 4-fold <15 5 8-fold
Assessment of Ca/PO4 disturbance* (CKD Mineral and Bone disorder) What to measure Calcium (corrected for albumin) Phosphate Alkaline phosphatase Bicarbonate PTH (Vitamin D3) How often? 12 monthly in CKD Stage 3 3 monthly in CKD Stage 4 *KDIGO position statement. Kid Intern 2006;69:1945
Goals of therapy for Ca/PO4 disturbance • Control s PO4 to <1.65 mmol/L • Keep s Ca in normal range (2.2-2.6 mmol/L) • Keeps Ca x PO4 <4mmol/L • Keep s PTH to ~2-3 times normal
Therapy for Ca/PO4 disturbance • Control s PO4 • Dietary restriction • Phosphate binders (prevent uptake) • Control s Ca • Adequate calcium intake • Calcitriol (increases uptake) • Control s PTH • Calcitriol • Cinacalcet • Parathyroidectomy