Muscular Dystrophy
Muscular Dystrophy. Omid yaghini. Congenital Muscular Dystrophy. Presentation : neonatal onset of severe weakness, delayed motor milestones, contractures Merosin negative/CMD A1 White matter hypodensities on brain scan but normal mental capacity

Muscular Dystrophy
E N D
Presentation Transcript
Muscular Dystrophy Omidyaghini
Congenital Muscular Dystrophy • Presentation: neonatal onset of severe weakness, delayed motor milestones, contractures • Merosin negative/CMD A1 • White matter hypodensities on brain scan but normal mental capacity • Diagnosis by muscle biopsy immunohistochemistry showing loss of α2-laminin (AR-chromosome 6q22-23)
Myotonic Muscular Dystrophy or Steinert’s disease • Presentation – adult with multiple systems affected • Primarily distal and facial weakness • Facial features: frontal balding in men, ptosis, low-set ears, hatchet jaw, dysarthria, swan neck, ^ shaped upper lip • Myotonia: worse in cold weather, after age 20 • Heart: conduction block – evaluate syncope • Smooth muscle: constipation, care with swallowing, gallstones, problems with childbirth, BP lability • Brain: learning disabilities, increased sleep requirement • Ophthalmology: cataracts • Endocrine: insulin resistance, hypothyroidism, testicular atrophy
Genetics: • Mothers can have adult or congenital onset offspring; fathers can have adult onset offspring • Parents may not be aware of own diagnosis • Myotonin gene is affected as well as adjacent transcription factor gene SIX 5 by CTG repeat in noncoding region of chromosome 19q13.3, and anticipation seen with increased repeats • Muscle biopsy with internalized nuclei, type 1 fiber atrophy, ring fibers, and sarcoplasmic masses • Congenital: severe form, initial respiratory distress after birth with ventilatory requirement or apnea, feeding difficulty, mental retardation, club feet, scoliosis, strabismus
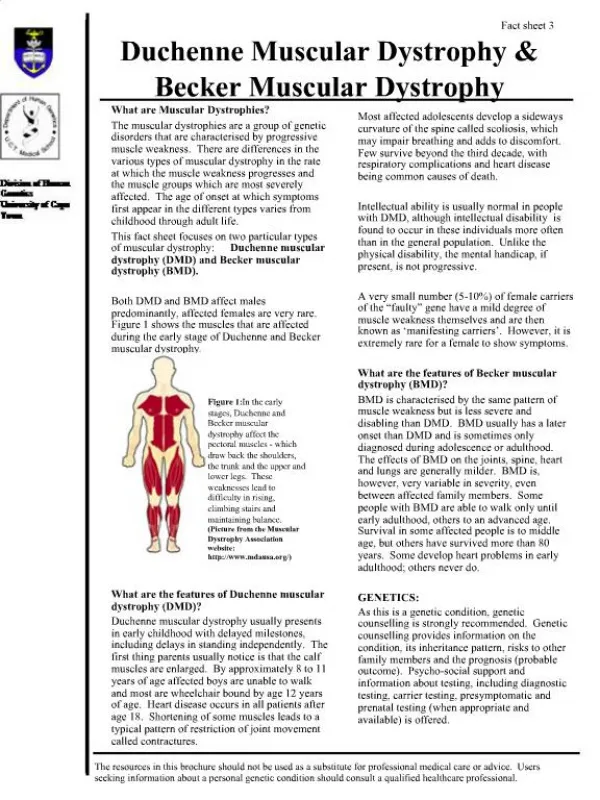
FascioScapularHumeral Muscular Dystrophy • Presentation: • Facial weakness with trouble blowing up a balloon, sipping through a straw, whistling, trouble closing the eyes at night, scapular winging that may be asymmetric, pain • May have absence of pectoralis, biceps, or brachioradialis • Also affected: mild high pitched hearing loss, retinal abnormalities, mental retardation in early onset • Genetics/Testing • Southern blot testing available (chromosome 4q35) for decrease in repeats normally present • Muscle biopsy may show lymphocytic infiltrates
Oculopharyngeal Muscular Dystrophy • Presentation: mid-adult with ptosis, facial muscle weakness with difficulty swallowing, proximal muscle weakness, may have extraocular muscle weakness, more common in French-Canadian and Hispanic population • Genetics • Muscle biopsy shows filamentous nuclear inclusions and ubiquitin containing vacuoles • Affects poly A binding protein 2 (PABP2) by expansion of a GCG repeat without anticipation seen – Southern blot (chromosome 14q11-13)
Limb Girdle Muscular Dystrophy • Presentation: variable age of onset with weakness and wasting of the limb-girdle • May have calf hypertrophy, involvement of scapular muscle and deltoid in sarcoglycanopathies • Many types involve dysfunctional sarcoglycans – transmembrane proteins of the DAP that interact with cytoplasmic proteins • Table 2 – types of LGMD
Emery-Dreifuss Muscular DystrophyScapuloperoneal MD • Presentation: stiff joints, shoulder and upper arm weakness, calf weakness, cardiac conduction defects and arrhythmias, contractures • Genetics • X-linked type affects emerin • Diagnose by protein analysis of leukocytes or skin fibroblasts • DNA testing available (chromosome Xq28) • AD affects lamin A or lamin C (chromosome 1q21) • Nuclear membrane proteins
Distal Muscular Dystrophy • Presentation: weakness in forearms, hands, and lower legs • clinically similar to a neuropathy but NCV normal • Muscle biopsy with autophagocytic vacuoles/ inclusion bodies • Table 3 – Types of DMD
Treatment - Medications • Steroids • Briefly increase strength, slow progression in dystrophinopathy for walking, arm use, and respiratory function • Weekend or 15-20/month as well as prednisolone/deflazacort may minimize SE • Dilantin and Tegretol raise the repolarization threshold and improve myotonia • Methylphenidate improves daytime somnolence in DM • Albuterol may help in FSH MD • Creatine and glutamine may help delay progression/improve energy in youngest with DMD
Treatment – future therapies • Genetic therapies • Repairing the mutated sequences • Using cell’s own repair mechanisms but adding template • Gentamicin trial for relaxation in stop codon recognition for DMD has not worked • Replacing the mutated sequences • Inserting truncated genes or whole gene with vector • Upregulation of similar functioning proteins • Utrophin in DMD
Therapy • Contracture prevention • Stretching exercises and postural changing • Stretch the most contracture prone groups (gastrocnemius, hip flexors, iliotibial bands, hamstrings) • AFO at night to supplement
Strengthening/conditioning/endurance • Goal is to maintain or improve muscle strength and maximize functional ability – slight improvement is possible • Additional goal is to avoid muscular damage by overwork or injury • No eccentric contraction or delayed soreness • Voluntary active exercise such as swimming/hydrotherapy or cycling in ambulatory children currently recommended
Mobility aids • Walking orthoses – KAFO • Standing frames, standing wheelchairs, swivel walker occasionally used • Walkers where arm strength less affected • Transfer board • Wheelchair – power needed for independence • Plan for indoor lift, van with lift, roll in shower • Improving daily activities of daily living • Physical and Occupational Therapy – teaching modified techniques • Antigravity orthoses are being developed to assist in daily living activities • Splinting and therapy to prevent hand contractures
Surgery • note the risk inherent to surgery – malignant hyperthermia • Palliative vs. rehabilitative • Tendon releases • Achilles • Need KAFO to walk post-op • Relieves pain and allow shoe wear • Hamstring and iliotibial band • Relieves hip and knee pain or contracture • Allows better gait compensation
Scoliosis – spine stabilization • Bracing is not effective with progressive neuromuscular disease • Timely correction of scoliosis is important for patient comfort and respiratory ability • Spine and scapular stabilization may aid function of arms • Ophthalmology • Deficient eye closure oculomaxillofacial MD and FSH MD may require artificial tears or tarsorrhaphy • Treatment for cataracts in Myotonic MD
Nutrition/GI • Overweight and underweight are common problems • Overweight impairs mobility • Underweight decreases strength & health • Protein and calorie supplements • Assess for dysphagia • Intestinal hypomotility in DMD, CMD, and myotonic dystrophy can require a bowel regimen to prevent constipation
Respiratory • Patients with morning headache, nightmares, excessive daytime somnolence, mental dullness, difficulty concentrating, increased colds, coughing, or pneumonia should undergo evaluation • Influenza vaccine and pneumococcal vaccine • In-exsufflator for airway clearance, cough assist • Pulmonologist, pulmonary function testing
Assisted noninvasive ventilation • Oxygen alone does not ventilate! • Positive pressure ventilation vs. volume ventilation with pressure limit • Assisted ventilation with tracheostomy • Talk to patient about degree of desired intervention when respiratory status first starts to decline and before an acute event • The goal is home ventilation • Cardiology • EKG – pacemaker for conduction defects and arrhythmias • Echocardiogram – afterload reduction, digoxin for cardiomyopathy
Osteopenia/Osteoporosis • Begins before walking stops, fractures may end walking • Worsened by steroids • Calcium supplements, Miacalcin may help • Psychology/Neuropsychological • Education – aid in planning • Special education may not be needed with accomodation and modifications • Progressive loss of function affects patient and family