Inflammatory Disorders
Inflammatory Disorders. Updated Fall 2011 by John Nation From the notes of Nancy Jenkins. Overview of Today’s Lecture. A & P Review Endocarditis- infection of the endocardial surface of the heart Myocarditis- a focal or diffuse inflammation of the myocardium

Inflammatory Disorders
E N D
Presentation Transcript
Inflammatory Disorders Updated Fall 2011 by John Nation From the notes of Nancy Jenkins
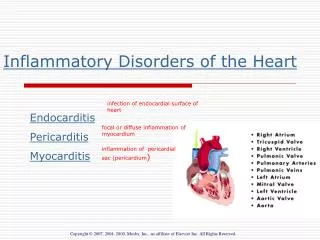
Overview of Today’s Lecture • A & P Review • Endocarditis- infection of the endocardial surface of the heart • Myocarditis- a focal or diffuse inflammation of the myocardium • Pericarditis- inflammation of the pericardial sac (the pericardium)
A- Aortic Valve B- Mitral Valve D- Tricuspid Valve - Pulmonary Valve
Anatomy and Physiology Review Blood enters the right atrium and moves through the _______ into the right ventricle. Blood then moves from the right ventricle into the pulmonary artery via the _________. A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve
Anatamy and Physiology Review (Cont’d) • After entering the left atrium via the pulmonary veins, blood moves through the _____ into the left ventricle. • Finally, it travels through the _____ and out of the heart. A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve
Infective Endocarditis • Infection of the inner layer of the heart • Usually affects the cardiac valves • Was almost always fatal until • development of penicillin • Around 15,000 cases diagnosed • annually in the U.S.
Causative Organisms • Causative organism more virulent • Streptococcus viridans • Staphylococcus aureus • Viruses • Fungi
Etiology and Pathophysiology • Vegetation • Fibrin, leukocytes, platelets, and microbes • Adhere to the valve or endocardium • Embolization of portions of vegetation into circulation
Etiology and Pathophysiology • Occurs when blood turbulence within heart allows causative agent to infect previously damaged valves or other endothelial surfaces
Endocarditis • Infection of the innermost layers of the heart • May occur in people with congenital and valvular heart disease • May occur in people with a history of rheumatic heart disease • May occur in people with normal valves with increased amounts of bacteria
Etiology/Pathophysiology • Endocarditis • When valve damaged, blood is slowed down and forms a clot. • Bacteria get into blood stream • Bacterial or fungal vegetative growths deposit on normal or abnormal heart valves
Classifications of Endocarditis • Acute Infective Endocarditis • Abrupt onset • Rapid course • Staph Aureus • Subacute Infective Endocarditis SBE • Gradual onset • Systemic manifestations • Prosthetic Valve Endocarditis
Risk Factors- endocarditis • Hx of rheumatic fever or damaged heart valve • Prior history of endocarditis • Invasive procedures- (introduce bacteria into blood stream) (surgery, dental, etc) • Recent Dental Surgery • Permanent Central Venous Access • IV drug users • Valve replacements
Nursing Assessment • Subjective Data • History of valvular, congenital, or syphilitic cardiac disease • Previous endocarditis • Staph or strep infection • Immunosuppressive therapy • Recent surgeries and procedures
Nursing Assessment • Functional health patterns • IV drug abuse • Alcohol abuse • Weight changes • Chills
Nursing Assessment • Diaphoresis • Bloody urine • Exercise intolerance • Generalized weakness • Fatigue • Cough
Nursing Assessment • Dyspnea on exertion • Night sweats • Chest, back, abdominal pain
Collaborative Care • Fungal and prosthetic valve endocarditis • Responds poorly to antibiotics • Valve replacement is adjunct procedure
Assesment endocarditis • Infection and emboli • Emboli-spleen most often affected (splenectomy) • Osler’s nodes- painful, red or purple pea-sized lesions on toes and fingertips • Splinter hemorrhages- black longitudinal streaks on nail beds • Janeway lesions- flat, painless, small, red spots on palms and soles • Roth spots- hemorrhagic retinal lesions • Murmur- 90% have murmurs • T above 101(blood cultures) and low-grade • Chills • Anorexia • Fatigue
Clinical Manifestations • Murmur in most patients • Heart failure in up to 80% with aortic valve endocarditis • Manifestations secondary to embolism Heart Sounds Assessment Video
Auscultating Heart Sounds • The aortic area or right sternal border (RSB) is at the right 2nd intercostal space, just under and to the right of the angle of Louis (sternal angle) • The pulmonic area or left upper sternal border (LUSB) is at the left 2 nd intercostal space • The tricuspid area or left lower sternal border (LLSB) is at the left fifth intercostal space • The mitral area or apex is at the PMI -- the 5th intercostal space in midclavicular line
Splinter hemorrhage • small areas of bleeding under the fingernails or toenails. • due to damage to capillaries by small clots
Janeway Lesions • flat, painless red spots on palms and soles
Osler’s Nodes • Painful, pea-size, red or purple lesions • On finger tips or toes Roth spots Osler’s nodes
Roth’s Spots • hemorrhagic retinal lesions
Diagnostic Tests • Blood Cultures- • Echocardiogram-TEE best- see vegetations • Other- WBC with differential, CBC,ESR, serum creatinine,CXR, and EKG
Medications • Antibiotics • IV for 2-8 weeks • Monitor peaks and troughs of certain drugs • Monitor BUN and Creat. • Unclear success of oral antibiotics if not a good candidate for IV. Oral antibiotics are considered when dealing with endocarditis: • Of the tricuspid valve • With a causative organism sensitive to oral agents • Long-term IV therapy difficult or impossible • Outpatient f/u can be arranged
Nursing Diagnoses • Risk for Imbalanced Body Temperature • Risk for Ineffective Tissue Perfusion-emboli • Ineffective Health Maintenance
Complications • Emboli (50% incidence) • Right side- pulmonary emboli (esp. with IV drug abuse- Why??) • Left side-brain, spleen, heart, limbs,etc • CHF-check edema, rales, VS • Arrhythmias- A-fib • Death .
Prevention • Eliminate risk factors • Patient teaching
Risk Stratisfication for IE High Risk- • Mechanical prosthetic heart valve • Natural prosthetic heart valve • Prior infective endocardititis • Valve repair with prosthetic material • Most congenital heart diseases Moderate Risk- • Valve repair without prosthetic material • Hypertrophic cardiomyopathy • Mitral valve prolapse with regurgitation • Acquired valvular dysfunction Low Risk- • Innocent heart murmurs • Mitral valve prolapse without regurgitation • Coronary artery disease • People with pacemakers/ defibrillators • Prophylactic antibiotics are generally recommended only for people in the “High Risk” category
Collaborative Care • Prophylactic treatment for patients having • Removal or drainage of infected tissue • Renal dialysis • Ventriculoatrial shunts • Dental, oral, or upper respiratory tract procedures
Myocarditis Myocarditis is an uncommon inflammation of the heart muscle (myocardium). This inflammation can be caused by infectious agents, toxins, drugs or for unknown reasons. It may be localized to one area of the heart, or it may affect the entire heart.