Download
1 / 1
10 likes | 177 Vues
No. 164. Uro-symphyseal fistulation after prostatic irradiation – an unrecognised but important complication. Bugeja S, Chaudhury I, Andrich D.E, Mundy A.R Institute of Urology, University College London Hospital s , UK. Posters Proudly Supported by: . Methods (cont)

E N D
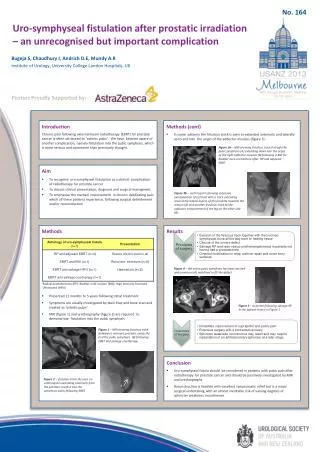
No. 164 Uro-symphysealfistulation after prostatic irradiation – an unrecognised but important complication Bugeja S, Chaudhury I, Andrich D.E, Mundy A.R Institute of Urology, University College London Hospitals, UK Posters Proudly Supported by: • Methods (cont) • In some patients the fistulous track is seen to extended anteriorly and laterally up to and into the origin of the adductor muscles (figure 3). Introduction Chronic pain following external beam radiotherapy (EBRT) for prostate cancer is often attributed to ‘osteitis pubis’. We have become aware of another complication, namely fistulation into the pubic symphysis, which is more serious and commoner than previously thought. Figure 3a – MRI showing fistulous track through the pubic symphysis (A) extending down into the origin of the right adductor muscles (B) following a BNI for bladder neck contracture after RP and adjuvant EBRT 3 • Aim • To recognise uro-symphyseal fistulation as a distinct complication of radiotherapy for prostate cancer • To discuss clinical presentation, diagnosis and surgical managment • To emphasise the marked improvement in chronic debilitating pain which all these patients experience, following surgical debridement and/or reconstruction 3 Figure 3b – urethrogram showing extensive extravasation of contrast with a track extending around the lateral aspect of the prostate towardsthe rectum (A) and another fistulous track to the adductor compartment of the leg on the other side (B) • Methods • Presented 11 months to 5 years following initial treatment • Symptoms are usually investigated by plain Xray and bone scan and treated as ‘osteitis pubis’ • MRI (figure 1) and urethrography (figure 2) are required to demonstrate fistulation into the pubic symphysis Results Figure4 – the entire pubic symphysis has been excised and omentum (A) mobilised to fill the defect 5 4 Radical prostatectomy (RP); Bladder neck incision (BNI); High Intensity Focussed Ultrasound (HIFU) Figure5 – outcome following salvage RP in the patient shown in Figure 1 Figure1 – MRI showing fistulous track between a remnant prostatic cavity (A) and the pubic symphysis (B) following EBRT and salvage cryotherapy. 1 A 2 • Conclusion • Uro-symphyseal fistula should be considered in patients with pubic pain after radiotherapy for prostate cancer and should be positively investigated by MRI and urethrography • Reconstruction is feasible with excellent symptomatic relief but is a major surgical undertaking with an almost inevitable risk of varying degrees of sphincter weakness incontinence Figure2 – fistulous track (A) seen on urethrogram extending anteriorly from the prostatic urethra into the symphysis pubis following EBRT A





