Download
1 / 1
20 likes | 391 Vues
Acute Exertional Paraspinal Muscle Compartment Syndrome: A “Can’t Miss” Diagnosis Nicholas Mazur DO, Daniel Falco DO, Faran Bokhari MD, FACS Department of Trauma Surgery, John H. Stroger Jr. Hospital of Cook County, Chicago, IL. Chief Complaint – Back Pain. Trauma Department Course.

E N D
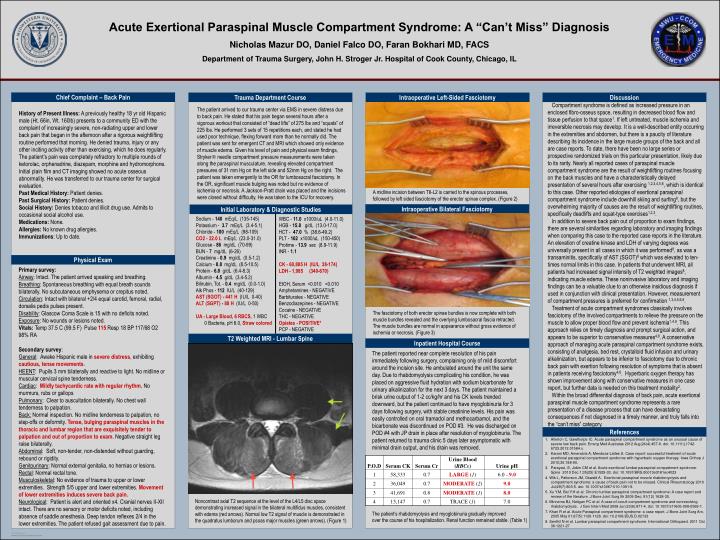
Acute Exertional Paraspinal Muscle Compartment Syndrome: A “Can’t Miss” Diagnosis Nicholas Mazur DO, Daniel Falco DO, Faran Bokhari MD, FACS Department of Trauma Surgery, John H. Stroger Jr. Hospital of Cook County, Chicago, IL Chief Complaint – Back Pain Trauma Department Course Intraoperative Left-Sided Fasciotomy Discussion Compartment syndrome is defined as increased pressure in an enclosed fibro-osseus space, resulting in decreased blood flow and tissue perfusion to that space1. If left untreated, muscle ischemia and irreversible necrosis may develop. It is a well-described entity occurring in the extremities and abdomen, but there is a paucity of literature describing its incidence in the large muscle groups of the back and all are case reports. To date, there have been no large series or prospective randomized trials on this particular presentation, likely due to its rarity. Nearly all reported cases of paraspinal muscle compartment syndrome are the result of weightlifting routines focusing on the back muscles and have a characteristically delayed presentation of several hours after exercising 1,2,3,4,5,6, which is identical to this case. Other reported etiologies of exertional paraspinal compartment syndrome include downhill skiing and surfing8, but the overwhelming majority of causes are the result of weightlifting routines, specifically deadlifts and squat-type exercises1,2,3. In addition to severe back pain out of proportion to exam findings, there are several similarities regarding laboratory and imaging findings when comparing this case to the reported case reports in the literature. An elevation of creatine kinase and LDH of varying degrees was universally present in all cases in which it was performed8, as was a transaminitis, specifically of AST (SGOT)8 which was elevated to ten-times normal limits in this case. In patients that underwent MRI, all patients had increased signal intensity of T2 weighted images8, indicating muscle edema. These noninvasive laboratory and imaging findings can be a valuable clue to an otherwise insidious diagnosis if used in conjunction with clinical presentation. However, measurement of compartment pressures is preferred for confirmation 1,3,4,5,6,8. Treatment of acute compartment syndromes classically involves fasciotomy of the involved compartments to relieve the pressure on the muscle to allow proper blood flow and prevent ischemia1,4,8. This approach relies on timely diagnosis and prompt surgical action, and appears to be superior to conservative measures4,8. A conservative approach of managing acute paraspinal compartment syndrome exists, consisting of analgesia, bed rest, crystalloid fluid infusion and urinary alkalinization, but appears to be inferior to fasciotomy due to chronic back pain with exertion following resolution of symptoms that is absent in patients receiving fasciotomy4,8. Hyperbaric oxygen therapy has shown improvement along with conservative measures in one case report, but further data is needed on this treatment modality2. Within the broad differential diagnosis of back pain, acute exertional paraspinal muscle compartment syndrome represents a rare presentation of a disease process that can have devastating consequences if not diagnosed in a timely manner, and truly falls into the “can’t miss” category. The patient arrived to our trauma center via EMS in severe distress due to back pain. He stated that his pain began several hours after a vigorous workout that consisted of “dead lifts” of 275 lbs and “squats” of 225 lbs. He performed 3 sets of 15 repetitions each, and stated he had used poor technique, flexing forward more than he normally did. The patient was sent for emergent CT and MRI which showed only evidence of muscle edema. Given his level of pain and physical exam findings, Stryker needle compartment pressure measurements were taken along the paraspinal musculature, revealing elevated compartment pressures of 31 mm Hg on the left side and 52mm Hg on the right. The patient was taken emergently to the OR for lumbosacral fasciotomy. In the OR, significant muscle bulging was noted but no evidence of ischemia or necrosis. A Jackson-Pratt drain was placed and the incisions were closed without difficulty. He was taken to the ICU for recovery. History of Present Illness: A previously healthy 18 yr old Hispanic male (Ht. 66in, Wt. 160lb) presents to a community ED with the complaint of increasingly severe, non-radiating upper and lower back pain that began in the afternoon after a rigorous weightlifting routine performed that morning. He denied trauma, injury or any other inciting activity other than exercising, which he does regularly. The patient’s pain was completely refractory to multiple rounds of ketorolac, orphenadrine, diazepam, morphine and hydromorphone. Initial plain film and CT imaging showed no acute osseous abnormality. He was transferred to our trauma center for surgical evaluation. Past Medical History: Patient denies. Past Surgical History: Patient denies. Social History: Denies tobacco and illicit drug use. Admits to occasional social alcohol use. Medications: None. Allergies: No known drug allergies. Immunizations: Up to date. A midline incision between T6-L2 is carried to the spinous processes, followed by left sided fasciotomy of the erector spinae complex. (Figure 2) Sodium - 140 mEq/L (135-145) Potassium - 3.7 mEq/L (3.4-5.1) Chloride - 100 mEq/L (98-109) CO2 - 22.0 L mEq/L (23.0-31.0) Glucose - 86 mg/dL (70-99) BUN - 7 mg/dL (6-26) Creatinine - 0.9 mg/dL (0.5-1.2) Calcium - 8.8 mg/dL (8.5-10.5) Protein - 6.8 g/dL (6.4-8.3) Albumin - 4.5 g/dL (3.4-5.2) Bilirubin, Tot. - 0.4 mg/dL (0.0-1.0) Alk Phos - 112 IU/L (40-129) AST (SGOT) - 441 H (IU/L 0-40) ALT (SGPT) - 88 H (IU/L 0-50) UA - Large Blood, 6 RBCS, 1 WBC 0 Bacteria, pH 6.0, Straw colored Intraoperative Bilateral Fasciotomy Initial Laboratory & Diagnostic Studies WBC - 11.0 x1000/uL (4.0-11.0) HGB - 15.8 g/dL (13.0-17.0) HCT - 47.0 % (38.6-49.2) PLT - 162 x1000/uL (150-450) Protime - 13.9 sec (8.9-11.9) INR - 1.1 CK - 60,885 H (IU/L 38-174) LDH - 1,985 (340-670) EtOH, Serum <0.010 <0.010 Amphetamines - NEGATIVE Barbiturates - NEGATIVE Benzodiazepines - NEGATIVE Cocaine - NEGATIVE THC - NEGATIVE Opiates - POSITIVE* PCP - NEGATIVE Physical Exam Primary survey:Airway: Intact. The patient arrived speaking and breathing.Breathing: Spontaneous breathing with equal breath sounds bilaterally. No subcutaneous emphysema or crepitus noted.Circulation: Intact with bilateral +2/4 equal carotid, femoral, radial, dorsalis pedis pulses present.Disability: Glascow Coma Scale is 15 with no deficits noted.Exposure: No wounds or lesions noted. Vitals: Temp 37.5 C (99.5 F) Pulse 115 Resp 18 BP 117/68 O2 98% RA Secondary survey:General: Awake Hispanic male in severe distress, exhibiting cautious, tense movements.HEENT: Pupils 3 mm bilaterally and reactive to light. No midline or muscular cervical spine tenderness.Cardiac: Mildly tachycardic rate with regular rhythm. No murmurs, rubs or gallopsPulmonary: Clear to auscultation bilaterally. No chest wall tenderness to palpation.Back: Normal inspection. No midline tenderness to palpation, no step-offs or deformity. Tense, bulging paraspinal muscles in the thoracic and lumbar region that are exquisitely tender to palpation and out of proportion to exam. Negative straight leg raise bilaterally. Abdominal: Soft, non-tender, non-distended without guarding, rebound or rigidity.Genitourinary: Normal external genitalia, no hernias or lesions. Rectal: Normal rectal tone.Musculoskeletal: No evidence of trauma to upper or lower extremities. Strength 5/5 upper and lower extremities. Movement of lower extremities induces severe back pain. Neurological: Patient is alert and oriented x4. Cranial nerves II-XII intact. There are no sensory or motor deficits noted, including absence of saddle anesthesia. Deep tendon reflexes 2/4 in the lower extremities. The patient refused gait assessment due to pain. The fasciotomy of both erector spinae bundles is now complete with both muscle bundles revealed and the overlying lumbosacral fascia retracted. The muscle bundles are normal in appearance without gross evidence of ischemia or necrosis. (Figure 3) T2 Weighted MRI - Lumbar Spine Inpatient Hospital Course The patient reported near complete resolution of his pain immediately following surgery, complaining only of mild discomfort around the incision site. He ambulated around the unit the same day. Due to rhabdomyolysis complicating his condition, he was placed on aggressive fluid hydration with sodium bicarbonate for urinary alkalinization for the next 3 days. The patient maintained a brisk urine output of 1-2 cc/kg/hr and his CK levels trended downward, but the patient continued to have myoglobinuria for 3 days following surgery, with stable creatinine levels. His pain was easily controlled on oral tramadol and methocarbamol, and the bicarbonate was discontinued on POD #3. He was discharged on POD #4 with JP drain in place after resolution of myoglobinuria. The patient returned to trauma clinic 5 days later asymptomatic with minimal drain output, and his drain was removed. References • Allerton C, Gawthorpe IC. Acute paraspinal compartment syndrome as an unusual cause of severe low back pain. Emerg Med Australas 2012 Aug;24(4):457-9. doi: 10.1111/j.1742-6723.2012.01584.x. • Karam MD, Amendola A, Mendoza-Lattes S. Case report: successful treatment of acute exertional paraspinal compartment syndrome with hyperbaric oxygen therapy. Iowa Orthop J 2010;30:188-90. • Parayavi, E, Jobin CM et al. Acute exertional lumbar paraspinal compartment syndrome. Spine 2010 Dec 1;35(25):E1529-33. doi: 10.1097/BRS.0b013e3181ec4023 4. Wik L, Patterson JM, Oswald A. Exertional paraspinal muscle rhabdomyolysis and compartment syndrome: a cause of back pain not to be missed. Clinical Rheumatology 2010 Jul;29(7):803-5. doi: 10.1007/s10067-010-1391-9. 5. Xu Y.M, Bai Y.H et al. Chronic lumbar paraspinal compartment syndrome: A case report and review of the literature. J Bone Joint Surg Br 2009 Dec; 91(12) 1628-30. 6. Minnema BJ, Neligan PC et al. A case of occult compartment syndrome and nonresolving rhabdomyolysis. J Gen Intern Med 2008 Jun;23(6):871-4. doi: 10.1007/s11606-008-0569-1. 7. Khan R et al. Acute Paraspinal compartment syndrome: a case report. J Bone Joint Surg Am, 2005 May 01;87(5):1126-1128. doi: 10.2106/JBJS.D.02133 8. Senthil N et al. Lumbar paraspinal compartment syndrome. International Orthopaed. 2011 Oct 36:1221-27 Noncontrast axial T2 sequence at the level of the L4/L5 disc space demonstrating increased signal in the bilateral multifidus muscles, consistent with edema (red arrows). Normal low T2 signal of muscle is demonstrated in the quadratus lumborum and psoas major muscles (green arrows). (Figure 1) The patient’s rhabdomyolysis and myoglobinuria gradually improved over the course of his hospitalization. Renal function remained stable. (Table 1)