Download
1 / 53
740 likes | 1.72k Vues
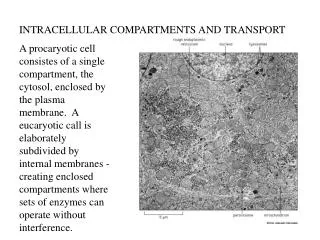
Lecturer name: Dr. Maha Arafah Lecture Date : -9-2012. (Foundation Block, Pathology). INTRACELLULAR ACCUMULATIONS and CALCIFICATION . Objectives. Understand the pathological changes leading to abnormal accumulations of pigments and other substances in cells.

E N D
Lecturer name: Dr. MahaArafah Lecture Date: -9-2012 (Foundation Block, Pathology) INTRACELLULAR ACCUMULATIONS and CALCIFICATION
Objectives • Understand the pathological changes leading to abnormal accumulations of pigments and other substances in cells. • List conditions and features of fatty change, haemosiderin, melanin and lipofuscin accumulations in cells. • Know the main types and causes of calcifications (dystrophic and metastatic).
Accumulation • Under some circumstances cells may accumulate abnormal amounts of various substances. • They may be harmless or associated with varying degrees of injury . • Cells may accumulate pigments or other substances as a result of a variety of different pathological or physiological processes.
Overview of Accumulation • May be found: • in the cytoplasm • within organelles (typically lysosomes) • in the nucleus • The accumulations can be classified as endogenous or exogenous. • Came to the cell through: • Synthesis by affected cells • Produced elsewhere.
Pathwaysof Accumulation Storage Diseases
Objectives • Understand the pathological changes leading to abnormal accumulations of pigments and other substances in cells. • List conditions and features of fatty change, haemosiderin, melanin and lipofuscin accumulations in cells. • Know the main types and causes of calcifications (dystrophic and metastatic).
(Steatosis) Fatty Change
Fatty Change • Fatty change is: any abnormal accumulation of triglycerides within parenchymal cells. • It is usually an early indicator of cell stress and reversible injury. • Site: • liver, most common site which has a central role in fat metabolism. • it may also occur in heart: anaemia or starvation (anorexia nervosa) • Other sites: skeletal muscle, kidney and other organs.
Causes of Fatty Change Steatosis may be caused by: • Toxins(most importantly: Alcohol abuse) • diabetes mellitus • Protein malnutrition (starvation) • Obesity • Anoxia
Starvation will increase this Hepatotoxins and anoxia (e.g. alcohol) by disrupting mitochondria and SER = Inhibit fatty acid oxidation • Defects in any of the steps of uptake, catabolism, or secretion can lead to lipid accumulation. CCl4 and protein malnutrition
The significance of fatty change • Depends on the cause and severity of the accumulation. • Mild it may have no effect on cellular function. • Severe fatty change may transiently impair cellular function
Light microscopy of fatty change • Early: small fat vacuoles in the cytoplasm around the nucleus. • Later stages: the vacuoles coalesce to create cleared spaces that displace the nucleus to the cell periphery • Occasionally contiguous cells rupture (fatty cysts)
Is Fatty liver reversible? • Fatty change is reversible except if some vital intracellular process is irreversibly impaired (e.g., in CCl4 poisoning),
Prognosis of Fatty liver • Mild: benign natural history (approximately 3% will develop cirrhosis • Moderate to sever: inflammation, degeneration in hepatocytes, +/- fibrosis (30% develop cirrhosis) • 5 to 10 year survival:67% and 59%
Other form of accumulation • Cholesteryl esters • These give atherosclerotic plaques their characteristic yellow color and contribute to the pathogenesis of the lesion • This is called atherosclerosis
Pigments are colored substances that are either: • exogenous, coming from outside the body, or • endogenous, synthesized within the body itself.
Exogenous pigment • They may be toxic and produce inflammatory tissue reactions or they may be relatively inert. • Indian ink pigments produce effective tattoos because they are engulfed by dermal macrophages which become immobilized and permanently deposited.
Exogenous pigment: carbon • The most common is carbon • When inhaled, it is phagocytosed by alveolar macrophages and transported through lymphatic channels to the regional tracheobronchial lymph nodes.
Exogenous pigment: carbon • Heavy accumulations may induce fibrosis ( coal workers' pneumoconiosis) Aggregates of the pigment blacken the draining lymph nodes and pulmonary parenchyma (anthracosis).
Endogenous Pigments • Hemosidren • Melanin • Lipofuscin
Hemosiderin ( iron) • is a hemoglobin-derived granular pigment that is golden yellow to brown and accumulates in tissues when there is a local or systemic excess of iron. • Hemosiderin pigments is composed of aggregates of partially degraded ferritin, which is protein-covered ferric oxide and phosphate. • It can be seen by light and electron microscopy
Hemosiderin • The iron ions of hemoglobin accumulate as golden-yellow hemosiderin. The iron can be identified in tissue by the Prussian blue histochemical reaction
Hemosiderin( iron) • Although hemosiderin accumulation is usually pathologic, small amounts of this pigment are normal. • Where? • in the mononuclear phagocytes of the bone marrow, spleen, and liver. • Why? • there is extensive red cell breakdown.
Hemosiderin • Local excesses of iron, and consequently of hemosiderin, result from hemorrhage. • Bruise: The original red-blue color of hemoglobin is transformed to varying shades of green-blue by the local formation of biliverdin (green bile) and bilirubin (red bile) from the heme
Hemosiderosis(systemic overload of iron) • is systemic overload of iron, hemosiderin is deposited in many organs and tissues • Site: liver, bone marrow, spleen, and lymph nodes • With progressive accumulation, parenchymal cells throughout the body (principally the liver, pancreas, heart, and endocrine organs) will be affected
Hemosiderosis • Hemosiderosis occurs in the setting of: • increased absorption of dietary iron • impaired utilization of iron • hemolytic anemias • transfusions (the transfused red cells constitute an exogenous load of iron). .
Effect of hemosiderosis • In most instances of systemic hemosiderosis, the iron pigment does not damage the parenchymal cells • However, more extensive accumulations of iron are seen in hereditary hemochromatosis with tissue injury including liver fibrosis, heart failure, and diabetes mellitus
Endogenous Pigments Melanin
Melanin • Melanin is the brown/black pigment which is normally present in the cytoplasm of cells at the basal cell layer of the epidermis, called melanocytes. • The function of melanin is to block harmful UV rays from the epidermal nuclei.
Melanin: Causes of accumulation • Melanin may accumulate in excessive quantities in benign or malignant melanocyticneoplasms and its presence is a useful diagnostic feature melanocytic lesions. • In inflammatory skin lesions, post-inflammatory pigmentation of the skin.
Endogenous Pigments Lipofuscin
Lipofuscin • "wear-and-tear pigment" is an insoluble brownish-yellow granular intracellular material that seen in a variety of tissues (the heart, liver, and brain) as a function of age or atrophy. • Brown atrophy
Lipofuscin • By electron microscopy, the pigment appears as perinuclear electron-dense granules
Degeneration Degeneration is used to describe pathological processes which result in deterioration (often with destruction) of tissues and organs. Examples: • Osteoarthritis : a degenerative joint disease in which gradual destruction and deterioration of the bones and joint occurs. • Alzheimer's disease : a degenerative neurological disease where there is a progressive deterioration in brain function. • Solar elastosis: UV-induced degeneration of the connective tissue in skin.
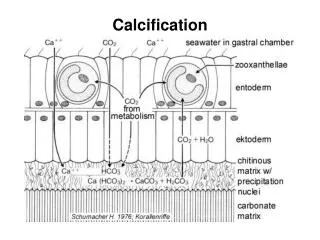
Pathologic calcification • is a common process in a wide variety of disease states • it implies the abnormal deposition of calcium salts with smaller amounts of iron, magnesium, and other minerals. • It has 2 types:
Types of Pathologic calcification • Dystrophic calcification: • When the deposition occurs in dead or dying tissues • it occurs with normal serum levels of calcium • Metastatic calcification: • The deposition of calcium salts in normal tissues • It almost always reflects some derangement in calcium metabolism (hypercalcemia)
Dystrophic calcification: • Encountered in areas of necrosis of any type. • E.g. a tuberculous lymph node is essentially converted to radio-opaque lesion due to calcification • E.g. in the atheromas of advanced atherosclerosis, associated with intimal injury in the aorta and large arteries
Although dystrophic calcification may be an incidental finding indicating insignificant past cell injury, it may also be a cause of organ dysfunction. • For example, • Dystrophic calcification of the aortic valves is an important cause of aortic stenosis in the elderly
Morphology of Dystrophic calcification • calcium salts are grossly seen as fine white granules or clumps, often felt as gritty deposits. • Histologically, calcification appears as intracellular and/or extracellular basophilic deposits. • In time, heterotopic bone may be formed in the focus of calcification.
Metastatic calcification • Metastatic calcification can occur in normal tissues whenever there is hypercalcemia.
Metastatic calcificationMain causes of hypercalcemia: • increased secretion of parathyroid hormone • destruction of bone due to the effects of accelerated turnover (e.g., Paget disease), immobilization, or tumors (multiple myeloma, leukemia, or diffuse skeletal metastases) • vitamin D-related disorders including vitamin D intoxication and sarcoidosis • renal failure, in which phosphate retention leads to secondary hyperparathyroidism.
Morphology of Metastatic calcification • Metastatic calcification can occur widely throughout the body but principally affects the interstitial tissues of the vasculature, kidneys, lungs, and gastric mucosa. • The calcium deposits morphologically resemble those described in dystrophic calcification.