Download
1 / 27
300 likes | 719 Vues
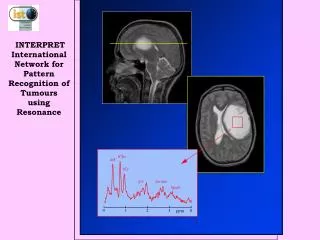
Applied Sciences Lecture Course. Glucose and Lactate metabolism in acute illness. Mahesh Nirmalan MD, FRCA, PhD Consultant, Critical Care Medicine Manchester Royal Infirmary. The initial arterial blood gas in A&E (30% O 2 ). pH: 7.19 Lactate: 12.6mmol.l -1

E N D
Applied Sciences Lecture Course Glucose and Lactate metabolism in acute illness Mahesh Nirmalan MD, FRCA, PhD Consultant, Critical Care Medicine Manchester Royal Infirmary
The initial arterial blood gas in A&E (30% O2) • pH: 7.19 Lactate: 12.6mmol.l-1 • PCO2: 3.1KPa Glucose: 12.5mmol.l-1 • PO2: 28KPa Na+: 140 mmol.l-1 • HCO3-: 12.3mmol.l-1 K+: 4.8mmol.l-1 • Base Excess (BE): -14.3mmol.l-1 • Cl-: 93mmol.l-1
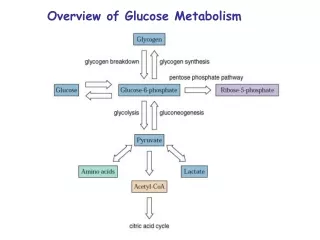
Overview of glucose metabolism What does Hyperglycaemia imply in acute illness? Role of Insulin and glucagon Catecholamines Overview of Lactate production and metabolism What does hyper lactataemia imply in the context of acute illness? Lactate± Metabolic acidosis Objectives
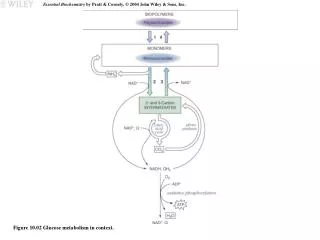
Glucose Liver Skeletal muscles Glucokinase Pentose Phosphate Shunt Glc-1- phosphate Glucose-6-P • Generation of Pentoses sugars • NADPH generation: Reduction of glutathione Glycolysis Pyruvate glycogen Complex carbohydrates → Oligosaccharides → MonosaccharidesDigestion • Serve as primary source of energy in the cell • Central to all metabolic processes • Teleologically a primitive metabolic pathway Cytosol - anaerobic
Cytosol Pyruvate Pyruvate dehydrogenase mitochondria (aerobic) Acetyl CoA FATTY ACIDS Reducing equivalents AMINO ACIDS Oxidative Phosphorylation: In mitochondria: Aerobic conditions Krebs cycle Oxidative Phosphorylation (ATP)
120 grams of glucose / day = 480 calories Site specific metabolic pathways Brain Capable of utilising alternate fuels: Time lag implies damage to higher functions
Direct effects of hyperglycaemia Effects of hyperglycaemia • Osmotic effect and cellular dehydration • Glycosuria: loss of glucose in urine • Osmotic diuresis and loss of body fluids • Long term effects • Lipogenesis • Vascular changes • Wound infections • Impaired wound healing
Diabetes is a complex metabolic diseaseAbsolute or relative insulin deficiencyHyperglycaemia is a common feature Plays only a minor role in the overall progression of disease
Rate limiting stage α to blood glucose within physiological range Site of action for sulphonylureas Insulin responses
Amino acids Metabolised→↑ATP Glucagon, GIP, Ach ↑Intracellular Ca2+ Sulphonylureas Inhibition of K+ - ATP channels Catecholamines Trauma, sepsis Somatostatin Inhibit exocytosis of Insulin Other modulators of insulin response + -
Role of Insulin on glucose metabolism • Promotes uptake and metabolism of glucose by muscles: At rest muscle depends on fatty acids rather than glucose for energy requirements • Exercise • Post prandial state • Storage of glycogen in muscles • Promotes liver uptake and storage • Increasing the activity of Glucokinase*** • Increasing the activity of glycogen synthase: Promotes glycogen synthesis • Inactivates liver phosphorylase: prevents glycogenolysis • Promotes conversion of glucose to fatty acids • Inhibits gluconeogenesis
Summary of blood glucose regulation • Normal person: narrowly controlled: 4.5-5 mmol.l-1 • Increases to 6.7-7.8 mg/dl during the 1st hour after meals • Feed back control: Normal within 2 hours • Starvation • Acute: Glycogenolysis and Gluconeogenesis • Chronic: Lipolysis and ketone body formation • The liver functions as an important blood glucose buffer system • Hypoglycaemia in Liver failure patients is always bad news • Insulin and glucagon the primary feed back system to maintain blood glucose • Sympathetic nervous system and Catecholamines • Delayed response from growth hormone and cortisol • Decreased utilisation of glucose • Greater fat utilisation
Insulin & Glucose response after injury • Claude Bernard: 1877:hyperglycaemia in haemorrhagic shock • 504 patients within 8hrs after injury • positive correlation between [glucose] and ISS • negative correlation between [Insulin] and ISS • Both responses most marked in severely injured patients with ISS>30 Hyperglycemia & hypoinsulinemia are essential features of severe injury and are mediated by the SNS? Frayn KN et al. Arch Emerg Med 1987;4:91-9
Hyperglycemia Increase in plasma osmolality by 20-30mOsmol Mobilisation of extracellular fluid : up to 500ml Jarhult J. Acta Physiol Scand 1973;89:213-226 Hyperglycaemia in injury and critical illness: an essential survival mechanism? Sympathetic activation Hypoinsulinaemia Corticosteroids, glucagon responses Increased glycogenolysis & gluconeogenesis
Tight control of blood sugar improves outcomeVan den Berghe, G. et al. 2001. N. Engl. J. Med.345:1359-1367 • Significant reduction in mortality in very unwell patients in whom blood sugar was controlled within a tight range • Less: nosocomial infections, acute renal failure, liver dysfunction, CIP, anaemia • Underlying mechanisms ??
X β-Oxidation FATTY ACIDS Ketone body formation Cytosol Pyruvate mitochondria (aerobic) Acetyl CoA Acetyl CoA produced from FFA is metabolised in the same way When Acetyl CoA cannot be produced from glucose →↑FFA oxidation Starvation, high fat diet: No carbohydrates Diabetes: carbohydrates cannot enter the cells Krebs cycle
Ketone body formation • 2 Molecules of Acetyl CoA condense→ acetoacetic acid • Acetoacetic acid→β-hydroxybutric acid & Acetone • Liver is the main source • Transported to and metabolised in most tissues • A normal physiological response • When excessive → ketosis • Starvation, very high fat diet, DKA • Decrease insulin and increase glucagon • Increased glucocorticoids
If the source of ketones is Acetyl CoA…..a common intermediate product …….why does ketosis occur only when FFA metabolism is switched on?
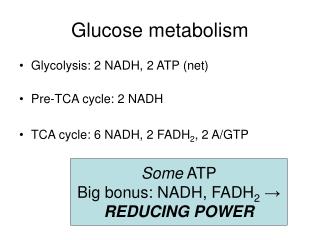
Aerobic Pyruvate dehydrogenase Kreb’s Cycle 2 ATP 34 ATP Oxidative phosphorylation Glucose Glycolysis NAD NADH, H+ + + 4H+ Lactate 2 Pyruvate 2 ATP Lactate dehydrogenase X Anaerobic
Glucose Metabolism under aerobic & anaerobic conditions AEROBIC ANAEROBIC Glucose Glucose 38 ADP 2 ADP 38 ATP 2 ATP H2O + CO2 LACTATE JVD-TMH
Glycogen LACTATE Gluconeo genesis 1500 mmol /day Glycolysis GLUCOSE
Acidosis Lactate- + H+ Lactic Acidosis Extracellular Intracellular Lactate production is buffered intracellularly Glucose Glycolysis NAD NADH, H+ Lactate 4H+ 2 ATP 2 Pyruvate Lactate dehydrogenase
Increased Lactate with normal pH → Usually implies a transient metabolic shift → Not of major consequence →No specific measures required Increased Lactate +Metabolic acidosis • Anaerobic metabolism • Tissue Hypoxia • Tissue hypo perfusion • Localised: mesenteric, coronary, limbs • Generalised: Shock, cardiac arrest • Sepsis • Hypo perfusion • Metabolic inhibition • Pyruvate dehydrogenase inhibition • Large tumours • Ischaemic core • It is not the lactate that kills
Glucose metabolism: Aerobic and anaerobic Hyperglycaemia is a physiological response to stress Role of Insulin, glucagon and catecholamine When excessive and prolonged may need to be controlled?? Diabetes: A complex endocrine disorder Naive to assess it purely in terms of hyperglycaemia Lactate is an important intermediary metabolite Hyper lactataemia : The significance should be assessed within the overall context of acid-base balance? Lactate: Usually but not always a marker of tissue hypoxia Summary