Download
1 / 82
830 likes | 1.06k Vues
Nur 4206 Management of patients with renal/urinary disorders. By Linda Self. Functions of the Kidney. Regulation of water excretion Regulation of electrolyte function Regulation of acid-base balance—retain HCO3- and excrete acid in urine Regulation of blood pressure--RAAS

E N D
Nur 4206Management of patients with renal/urinary disorders By Linda Self
Functions of the Kidney • Regulation of water excretion • Regulation of electrolyte function • Regulation of acid-base balance—retain HCO3- and excrete acid in urine • Regulation of blood pressure--RAAS • Regulation of RBCs • Vitamin D synthesis
Functions of Kidney cont. • Secretion of prostaglandin E and prostacyclin which cause vasodilation, important in maintaining renal blood flow • Excretion of waste products-body’s main excretory organ. Urea, creatinine, phosphates, uric acid and sulfates. Drug metabolites.
Hormones influencing renal function • Renin—raises BP • Bradykinins—increase blood flow and vascular permeability • Erythropoietin • ADH • Aldosterone—promotes sodium reabsorption and potassium excretion • Natriuretic hormones—released from the cardiac atria and brain.
Risk factors for renal or urologic disorders • Hypertension • Diabetes mellitus • Immobilization • Parkinson’s disease • SLE • Gout • Sickle cell anemia, multiple myeloma • BPH • Pregnancy • SCI
Gerontologic Considerations • GFR decreases following 40 years with a yearly decline of about 1 mL/min • Renal reserve declines • Multiple medications can result in toxic metabolites • Diminished osmotic stimulation of thirst • Incomplete emptying of bladder • Urinary incontinence
Urinalysis and culture • Sp. Gravity—1.005-1.020 • Microscopic examination for protein, RBCs, ketones, glycosuria, presence of bacteria, general appearance and odor • Leukocyte esterase—enzyme found in WBCs • Nitrites –bacteria convert nitrates to nitrites • Osmolality—accurate measurement of the kidney’s ability to concentrate urine. Normal range is 500-1200 mOsm/kg. • Culture important in ‘Id’ing pathogen
Urine tests • Albuminuria—albumin in urine not measurable by dipstick • Normal values in freshly voided sample should range between 2.0-20 for men and 2.8-28 for women. Higher levels indicate microalbuminuria. • Can also be determined by 24h specimen
Renal Function tests • Urine osmolality—indication of concentrating ability, changes seen early in disease processes • Creatinine clearance—tests clearance of creatinine in one min. Reflects GFR. • Serum creatinine—measures effectiveness of renal function. 0.6 to 1.2 mg/dL • Urea nitrogen—also indicator of renal function. 7-18 mg/dL. Measures renal excretion of urea nitirogen, a byproduct of protein metabolism. Is not always elevated with kidney disease. Not best indicator of renal function.
Renal function tests cont. • Liver must function properly to produce urea nitrogen. BUN levels indicate the extent of renal clearance of this nitrogenous waste product. • May see elevation of BUN with bleeding into tissues or from rapid cell destruction from infection/steroids
Renal Function Tests • Ratio of BUN to creatinine distinguishes between renal and non-renal factors causing elevations • Dehydration can affect the BUN • When blood volume is down, or BP is low, BUN level rises more rapidly than creatinine level.
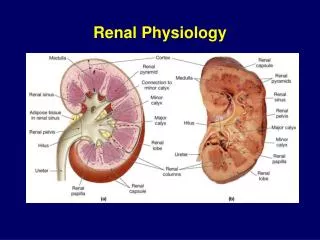
GFR • Volume of fluid filtered from renal glomerular capillaries into Bowman’s capsule per unit of time • Generally expressed in ml/minute • Normal GFR generally is 125mL/minute
Calculation of GFR—complex and differing formulas • Cockcraft-Gault formula • Modification of Diet in Renal Disease Study Group formula (MDRD) • Schwartz formula • Starling equation
No common pathologic condition, other than renal disease, increases the serum creatinine level • Serum creatinine does not increase until at least 50% of renal function is lost
Creatinine Clearance • Is a calculated measure of glomerular filtration rate. Is best indicator of overall kidney function. • Based on 24 hour urine collection • Midway will obtain serum creatinine. Serum creatinine levels vary with age, gender and body muscle mass • Calculate: (Volume of urine X urine creatinine) Divided by serume creatinine
Imaging Studies • KUB • Ultrasonography • CT • MRI • Nuclear scans • IV urography—IVP. NPO before. Bowel prep. Nephrotoxic agent. Metformin. • VCUG
Urologic Endoscopic Procedures • Cystoscopy • Ureteral brush biopsy • Kidney biopsy • Urodynamic tests—cystometrogram. Measures detrusor muscle function.
Glomerular Diseases • Antigen-antibody complexes form in blood and become trapped in glomerular capillaries • Induce an inflammatory response • Manifested by proteinuria, hematuria, decreased GFR and alteration in excretion of sodium • Acute and chronic glomerulonephritis • Nephrotic syndrome
Infectious causes • Staph, klebsiella, CMV, mono, hep B, mycoplasma, group A beta-hemolytic strep
Clinical Manifestations of acute glomerular nephritis • Hematuria • Edema • Azotemia-accumulation of nitrogenous wastes • Urine appearance may be cola colored • Hypertension • Hypoalbuminemia • Hyperlipidemia • Rising BUN and creatinine
Complications • Hypertensive encephalopathy • Heart failure • Rapid decline in renal function can occur to ESRD
Management • Treat s/s such as elevated BP • Check GFR by 24h urine for creatinine clearance • ANA • Treat streptococcal infection with antibiotics, preferably PCN • Corticosteroids • Immunosuppressants • Limit dietary protein, increase CHO • Restrict sodium • May progress to chronic glomerulonephritis, will treat as in CKD
Nephrotic Syndrome • Is not a specific glomerular disease • Is a syndrome with a cluster of findings that include: • Marked increase in protein in urine (especially albumin) • Hypoalbuminemia • Edema • High serum cholesterol and LDL
Nephrotic Syndrome • A condition of increased glomerular permeability • Results in massive protein loss • Often linked genetically or r/t immune/inflammatory process • Caused by chronic glomerulonephritis, diabetes mellitus with glomerulosclerosis, amyloidosis, lupus, multiple myeloma and renal vein thrombosis • Major manifestation is edema • Hallmark is albuminuria exceeding 3.5g/day
Complications of nephrotic syndrome • Massive proteinuria • Hypoalbuminemia • Edema • Lipiduria • Hyperlipidemia • Increased coagulation • Renal insufficiency
Treatment of nephrotic syndrome • Renal biopsy to determine specific cause • Steroids • Immunosuppressive agents • ACEIs can decrease proteinuria • Cholesterol lowering agents • Heparin to reduce coagulability • Limit sodium intake
Acute Renal Failure • Reversible clinical syndrome whereby there is sudden and pronounced loss of kidney function • Occurs over hours to days • Results in kidneys failure to excrete nitrogenous wastes
Causes of Acute Renal Failure Intrarenal actual parenchymal damage • Prolonged renal ischemia from myoglobinuria (rhabdo, trauma, burns), hemoglobinuria (transfusion reaction, hemolytic anemia) • Nephrotoxic agents like aminoglycosides, radiopaque contrast, heavy metals, solvents, NSAIDs, ACEIs, acute glomerulonephritis
Causes of Acute Renal Failure Prerenal 60-70% of cases • Volume depletion as seen in hemorrhage, renal losses from diuretics, GI losses from vomiting, diarrhea • Impaired cardiac output 2ndary to MI, heart failure, dysrhythmias, cardiogenic shock • Vasodilation from sepsis, anaphylaxis, antihypertensive meds
Causes of acute renal failure Postrenal Urinary tract obstruction by calculi, tumors, BPH, blood clots
Phases of Acute Renal Failure • Initiation occurs with the insult • Oliguria with urinary output less than 400ml/24h . rising potassium, BUN, Cr. Not responsive to fluid challenges. • Diuresis period— gradual increase in urinary output. Beginning recovery. Renal function gradually improves • Recovery—may take 3-12 months. May have permanent reduction in functioning of 1%-3%.
Key features of ARF • Prerenal-hypotension, tachycardia, decreased CO, decreased urinary output, lethargy • intrarenal and postrenal—oliguria or anuria, hypertension, tachycardia, SOB, orthopnea, n/v, generalized edema and weight gain, lethargy, confusion
Laboratory Profile of ARF • Elevated BUN and creatinine • Sodium retention but may be deceptive due to water retention • Potassium increased • Phosphorus increased • Calcium decreased • H&H decreased • Sp. Gravity decreased and fixed
Management • Objectives : Restore normal chemical balance and prevent complications until restoration of renal function • Identify and treat underlying cause • Maintain fluid balance—wts, serial CVP readings, BP, strict I&O • May give Mannitol, Lasix or Edecrin • May need temporary dialysis
Management • If prerenal, fluid challenges and diuretics to enhance renal blood flow • Oliguric renal failure, low dose dopamine. Calcium channel blockers may be used to prevent influx of calcium into kidney cells, maintains cell integrity and increase GFR
Management • Hyperkalemia—closely monitor electrolytes • Kayexalate/Sorbitol—may need Flexiseal • IV dextrose, insulin and calcium may help shift K+ • Cautious administration of any medication that can be nephrotoxic • Monitor ABGs and acid-base balance • Monitor phosphate levels
Nutritional Therapy • Azotemia and uremia are directly related to the rate of protein breakdown • Dietary proteins are individualized to each patient. Is a catabolic state and if insufficient intake, patient may lose up to 0.5-1 pounds daily. Encourage high CHO. Protein needs for non-dialysis patients need 0.6g/kg of body weight • Dialysis patients will need 1-1.5g/kg • Fluid restriction=urine volume plus 500ml
Role of nurse • Monitor fluid and electrolyte balance • Reduce metabolic demands • Promote pulmonary function • Prevent infection • Provide skin care • Provide support
Chronic Renal Failure (End-stage renal disease) • Progressive, irreversibe deterioration in renal function • Causation: #1 diabetes mellitus, hypertension, glomerulonephritis, pyelonephritis, polycystic kidney disease, vascular disorders, others • Uremia---collection of nitrogenous wastes normally excreted by the kidneys. S/S include: HA, seizures, coma, dry skin, rapid pulse, elevated BP, scanty urine, labored breathing
Kidney changes • Nephrons hypertrophy and work harder until 70-80% of renal function is lost • Nephrons could only compensate by decreasing water reabsorption thus: • Hyposthenuria—loss of urine concentrating ability occurs • Polyuria—increased urine output • Then isosthenuria—fixed osmolality • Gradual decline in urinary output
Stages of Renal Failure • GFR greater than or equal to 90mL/min/1.73 m2. Kidney damage w/normal or increased GFR • GFR = 60-89, mild decrease in GFR • GFR = 30-59, moderate decrease in GFR • GFR = 15-29. severe decrease in GFR • GFR < 15. Kidney failure
Clinical Manifestations • Every body system is affected • CV—hypertension (RAAS), heart failure, pulmonary edema, pericarditis, MI • Pulm.—crackles, Kussmaul, pleuritic pain • Derm—severe pruritus, uremic frost (urea crystals) • GI—n/v, anorexia, uremic fetor (ammonia odor to breath), constipation or diarrhea • Neurologic—LOC changes, confusion, seizures, agitation, neuropathies, RLS
Clinical Manifestations • Hematologic—anemia, thrombocytopenia • Musculoskeletal—muscle cramps, renal osteodystrophy, bone pain, bone fractures • Metabolic changes—urea and creatinine, sodium, potassium, acid-base, calcium and phosphorus