Skin Wounds Classification
Skin Wounds Classification. Chapter 16 (pages 328-332). Soft Tissue Injuries. Trauma that happens to the skin is visually exposed Categorized as a skin wound Defined as a break in the continuity of the soft parts of body structures caused by a trauma to these tissues

Skin Wounds Classification
E N D
Presentation Transcript
Skin Wounds Classification Chapter 16 (pages 328-332)
Soft Tissue Injuries • Trauma that happens to the skin is visually exposed • Categorized as a skin wound • Defined as a break in the continuity of the soft parts of body structures caused by a trauma to these tissues • Mechanical forces include: • Friction, scraping, compression, tearing, cutting, penetrating
Abrasion • Skin scraped against a rough surface • Several layers of skin are torn loose or totally removed • Usually more painful than a deeper cut b/c scraping of skin exposes millions of nerve endings
Abrasion—Treatment • Wash wound to remove all dirt and debris • Soap and water or hydrogen peroxide • Scrub wound if particles of dirt, rocks, or tar embedded • Leave open to air, unless oozing of fluid or blood • Apply antibiotic ointment to inhibit infections • Scrapes scab over quickly
Abrasion—Treatment • Loose skin flaps my form natural dressing; if flap dirty remove with clean nail clippers • Check on date of last tetanus immunization • Watch for signs of infection • Seek medical attention if any of following: • Pain increases after several days • Redness/red streaks appear beyond edges of wound • Swelling • Purulent drainage
Laceration • Flesh irregularly torn; cut or tear in the skin • Minimal bleeding, minimal pain, & no numbness or tingling • Cuts ≤ 0.25” (6mm) deep and 0.5” (1.3cm) long & have smooth, edges can be treated at home • Deeper lacerations should be treated by physician (stitches)
Laceration—Treatment • Cleaned with soap and water • Irrigate with clean water to remove debris • Do NOT use alcohol, iodine, or peroxide as it may cause further damage and slow healing process • Stop bleeding • Cover wound with sterile gauze • Apply direct & constant pressure (15min+)
Laceration—Treatment • Once wound cleaned, antibiotic ointment may be applied to reduce risk of infection & aid healing • Change sterile dressing daily as needed • Bruising and swelling are normal • Apply ice to site • Elevate area above level of heart • Contact a physician if: • Laceration more than 0.25” (6mm) deep and 0.5” (1.3cm) long • The wound is in area where wound by be opened by simple movement of body part • Wound on face, eyelids, or lips • Deep cuts on palm, finger, elbow or knee • Loss of sensation or ROM of body part as result of cut
Laceration—Treatment Stitches Steri-Strips®
Avulsion • Layers of skin torn off completely or only flap of skin remains • Same mechanism as laceration, but to extent that tissue is completely ripped from it’s source • May be considerable bleeding
Avulsion—Treatment • Clean wound with soap and water • If flap of skin remains connected replace skin in its original position • If deep avulsion, seek medical attention for stitches • If large piece of skin torn off place in plastic bag and put on ice • Skin should not get frozen or soaked in water • Take skin in plastic bag to doctor; may be able to save and replace torn-off piece
Puncture Wound • Penetration of skin by sharp object • Nails, tacks, ice picks, knives, teeth, needles • May be small in diameter and not seem serious • Do require treatment by physician • Can become infected easily b/c dirt and germs carried deep in the tissue
Puncture Wound—Treatment • Find out if part of object that caused wound still in the wound • i.e. lead from a pencil • Determine if other tissues have been injured by the object • Blood vessels, nerves, tendons, ligaments, bones, internal organs • Prevent infections • Bacterial skin infections, tetanus, infections in deeper structures (bones and joints)
Puncture Wound—Treatment • Risk of infections increases if: • wound was exposed to soil (may contain tetanus or other bacteria) • went through sole of shoe (↑ risk of bacterial infection that is difficult to treat) • injected into skin under high pressure • i.e. nail from nail gun, paint from high-pressure paint sprayer • Physician should be consulted if object penetrated deeply
Contusion • A blow compresses or crushes the skin surface and produces bleeding under the skin • Does not break skin • Bruising due to injury to blood vessels • Most mild and respond well to RICE
Contusion—Signs & Symptoms • Swelling • Pain to touch • Redness • Ecchymosis • accumulation of blood in skin & subcutaneous tissue more than one cm in diameter • General term=bruising • Result of bleeding; clotting or bleeding disorders • Bluish lesion at earliest stages of onset
Contusion—Treatment • Careful monitoring • Anti-inflammatory oral medications • Compressive dressing • Ice • Modalities to ↓ ecchymosis, ↓ swelling, ↑ ROM • Myositis ossificans: calcification that forms within muscle • Requires surgical intervention
Blister • Continuous rubbing over the surface of the skin causes a collection of fluid below or within the epidermal layer
Blister—Treatment • Wash area thoroughly • Use sterile blade to cut small hole in blister • Squeeze out clear fluid • Do not remove skin • Prevention: • Wear work gloves • Break in new shoes • Petroleum jelly/skin lube • Adhesive bandage
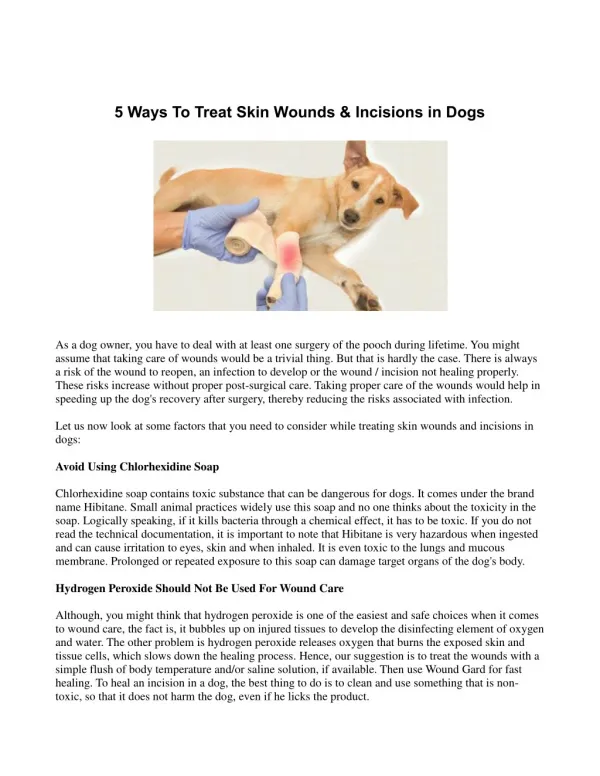
Incision • Skin has been sharply cut • Surgical cut made in skin or flesh
Incision—Treatment • Remove bandage day after surgery; replace daily or as needed • Normal for edges of healing incision to be slightly red • Call physician if: • redness increases/spreads more than half an inch • pus in incision • more than mildly tender or painful
Incision—Treatment • Keep incision clean & dry for several days after surgery • Non-absorbable sutures or staples must be kept dry until doctor removes • Steri-strips® should be kept dry 4-5 days • On face, hands, arms: take showers or tub baths along as affected area stays dry
Wound Care • Irrigate with clean, cool water to wash away foreign particles • Gentle wash with mild soap (superficial cuts only) • Minor cuts/abrasions should be washed, dried with sterile gauze sponge, and treated with first aid cream • Apply dry, sterile bandage, large enough to cover entire injury
Wound Care • Clean bandage should be applied daily • Athlete should be instructed on how to clean & manage wound • Athlete should check for signs of infection: • Redness • Swelling • Increased pain • Oozing of pus • Increase body temperature
Care of Open Wounds • Chart in Arnheim—p 928
Skin Infections • Skin always has some amount of bacteria, fungus, and viruses living on it • Skin infections occur when there are breaks in the skin and the organisms have uncontrolled growth • It is more important to understand the potential for infection rather than placing a name on the skin problem
Skin Infections • Bacteria—can be cured • Staphlococcus • Including MRSA & Impetigo • Streptococcus • Fungal—can be cured • Ringworm • Viral—cannot be cured, but can be treated • Herpes • Warts • Molluscum contagiosum
When to Worry • Lesions with an irregular border • Raised skin lesions • “wet” or “moist” lesions • Lesions that have different colors within the lesion • Bright red colored lesions are more of a problem compared to faded lesions • Lesions that are warmer compared to other skin • Inflammation & irritation around skin lesion • Prior history of infectious skin lesion • Skin abrasions • Deeper or more traumatic break in skin, higher risk for subsequent infection
Skin Infections • The right antibiotic is required to cure a specific bacterial skin infection • Antibiotics for bacteria will not improve fungal or viral infections • Bacterial infections can be the fastest growing infections • Thus the most easily spread among athletes
Staph • Infection caused by Staphylococcus bacteria • About 25% of people normally carry staph in the nose, mouth, genitals, and anal areas • Infection begins with a little cut gets infected with bacteria • Range from a simple boil to antibiotic-resistant infections to flesh-eating infections • Difference is: • the strength of the infection • How deep it goes • How fast it spreads • How treatable it is with antibiotics
MRSA • Methicillin resistant Staphylococcus aureus • Resistant to certain antibiotics most are skin infections • Methicillin, oxacillin, penicillin, amoxicillin • More severe or potentially life-threatening occur most frequently among patients in healthcare settings
Symptoms of MRSA Skin Infections Severe Infections Potentially life-threatening Blood stream infections Surgical site infections Pneumonia Signs & symptoms vary by type and stage of infections • Appear as pustules or boils • Red • Swollen • Painful • Pus or other drainage • First look like spider bites or bumps • Occur at sites of visible skin trauma
Causes of MRSA • Spread by having contact with someone’s skin infection or personal items they’ve used • Spread in places where people are in close contact • Close skin-to-skin contact • Openings in the skin (cuts or abrasions) • Contaminated items & surfaces • Crowded living conditions • Poor hygiene
Personal Prevention of MRSA • Good hygiene • Keep hands clean—wash with soap and water thoroughly • Keep cuts and scrapes clean & covered with a bandage • Avoid contact with other’s wounds/bandages • Avoid sharing personal items i.e. towels, razors
Prevention of MRSA in Athletics • Practice good personal hygiene • Keep hands clean • Shower after exercise • Do not share soap or towels • Wash uniform & clothing • Take care of your skin • Cover abrasions/cuts • Change bandages regularly • Do not share items that come in contact with your skin • Towels & razors • Ointments • Take precautions with common surfaces & equipment • Use barrier between skin & surface (towel, clothing)
Diagnosis & Testing of MRSA • Culture must be obtained • Small biopsy of skin • Drainage from infected site • Blood • Urine • Sent to microbiology laboratroy • Tested for S. aureus infection • Determine which antibiotics will be effective
Treatment of MRSA • Antibiotic to drain infection • DO NOT attempt to treat yourself! • Includes popping, draining, using disinfectants on area • If you think you have an infection: • Cover affected skin • Wash hands • Contact physician
MRSA Statistics • 2005: estimated 94,360 people develop serious MRSA infection • Approx 18,650 person died during hospital stay related to these serious MRSA infections • About 85% of all invasive MRSA infections were associated with healthcare (2/3 outside of hospital) • About 14% of all infections occurred in persons without obvious exposures to healthcare
Impetigo • Mild itching & soreness • Eruption of small vesicles and/or pustules that rupture to form honey-colored crusts • Combo of 2 bacteria that spread rapidly when athletes in close contact with one another • Responds rapidly to proper treatment • Thorough cleansing of crusted area • Application of topical antibacterial agent
Impetigo—Causes • Caused by streptococcus (strep) or staphylococcus (staph) bacteria • MRSA becoming common cause • May occur on skin where there is no visible break • Most common in children, particularly unhealthy living conditions • Infection carried in fluid that oozes from blisters
Impetigo—Symptoms • Single or many blisters filled with pus • Easy to pop • When broken leave a reddish raw-looking base • Itching blister • Filled with yellow or honey-colored fluid • Oozing and crusting over • Rash • Skin lesions on face, lips, arms, or legs • Swollen lymph nodes near infection
Folliculitis • Inflammation of a hair follicle • Starts when hair particles damaged by friction • Clothing, blockage of follicle, shaving • Frequently become infected • Bacteria Staphylococcus (staph) • Painless or tender pustule (pimple) • May crust over • Rash or itching