Download
1 / 17
180 likes | 833 Vues
Surgical Treatment of Thoracic Outlet Syndrome. Mary Meek, M.D. University of Arkansas for Medical Sciences. Learning Objectives. Identify pertinent normal and abnormal anatomy related to the thoracic outlet Understand the commonly used surgical techniques

E N D
Surgical Treatment of Thoracic Outlet Syndrome Mary Meek, M.D. University of Arkansas for Medical Sciences
Learning Objectives • Identify pertinent normal and abnormal anatomy related to the thoracic outlet • Understand the commonly used surgical techniques • Identify the accepted surgical indications • Discuss the controversies surrounding TOS surgery
Overview • Normal anatomy • Abnormal anatomy • History of surgical procedures • Common surgical procedures • Accepted indications • Controversies
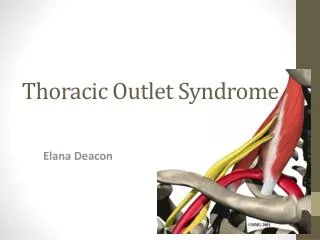
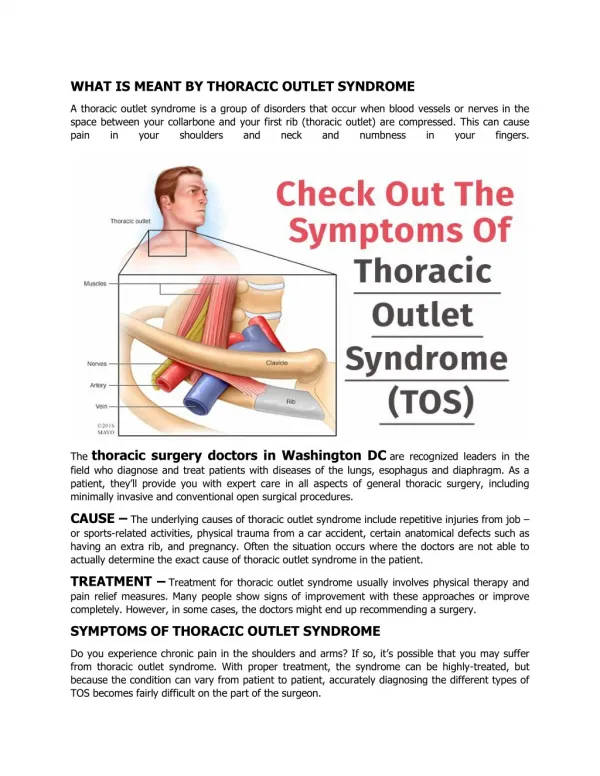
Normal thoracic outlet • Interscalene triangle • Costoclavicular triangle • Subcoracoid Space
Interscalene Triangle • Brachial plexus and subclavian artery pass posterior to anterior scalene • Subclavian vein passes anteriorly to anterior scalene • Common area of compression
CostoclavicularTriange • Middle 1/3 of clavicle
Subcoracoid Space • Under coracoid process deep to pectoralis minor
Muscular and fibrous causes of compression • Anterior Scalene • Middle Scalene • Pectoralis Minor • Costocoracoid ligament • Costoclavicular membrane • Subclavius muscle
Bony Abnormalities • 1st rib • Cervical rib • Long transverse process • Abnormal clavicle
History • 1742 Hunauld identified cervical rib as a cause of TOS • 1861 Coote performed the first cervical rib resection • 1916 Murphy published results of 1st rib resection
Common Surgical Procedures • Transaxillary approach • Anterior approach (Supra or Infraclavicular) • Posterior approach
Transaxillary approach • Preferred for neurogenic and venous TOS • Roos 1966 : 15 patients, anterior & middle scalene, rib, sympathectomy • “Advantage”: scar, no muscle splitting, complete rib visualization, proximal vessel control
Anterior approach • Preferred for arterial lesions • Preferred by some other surgeons (Eidt, personal communication)
Posterior approach • Primary for lower root decompression • Common for re-operation in particular to remove rib stump when initial resection is “incomplete”
Accepted indications for surgery • Definite anatomic abnormalities • Cervical rib • Abnormal insertion of costoclavicular ligament (common in Paget-Schroetter) • Vascular issues • Arterial aneurysms, embolic phenomenon • Paget-Schroetter • Nerve Conduction Velocity (NCV) < 60m/s
Controversies • Neurological symptoms • Surgeons diagnose TOS 100x more than neurologists • NCV between 60-85 m/s • Traumatic causes • Re-operation • “softer” abnormalities • Anterior Scalene spasm • Raynaud’s phenomenon
Summary • Definite anatomic abnormalities that can be cured by surgical resection • Common approaches are transaxillary and anterior (supraclavicular/infraclavicular) • “A chance to cut is a chance to cure” • Radiologist can be helpful with diagnosis (MRI, venography, sympathetic block) and therapy (thrombolysis)