Download
1 / 22
220 likes | 335 Vues
The special challenges of HIV prevention trials. EATG Meeting Brussels, Belgium. Lori Heise Global Campaign for Microbicides. Overview of the Day. Intro to prevention trials Participatory exercise Basics of ethical reasoning Balancing risks and benefits Lunch Standard of Care

E N D
The special challenges of HIV prevention trials EATG Meeting Brussels, Belgium Lori Heise Global Campaign for Microbicides
Overview of the Day • Intro to prevention trials • Participatory exercise • Basics of ethical reasoning • Balancing risks and benefits • Lunch • Standard of Care • Vaccine case study • Access to Treatment • Tenofovir case study
What is the Global Campaign? • An international coalition of NGOs working collaboratively to: • Raise awareness and mobilize political will for increased funding for microbicide research and eventual access; • Create a supportive policy and user environment for the timely development, introduction and use of new prevention technologies; and • Ensure that as science proceeds, the public interest is protected and the rights and interests of trial participants, users, and communitiesare fully represented and respected.
GCM Role in Ethics • GCM goals viz a viz ethics: • Help give voice to community and civil society perspectives on trial design and ethics issues • Help forge consensus around ethical debates that could delay progress • Negotiate difficult line between urgency of the HIV epidemic and maintaining rigorous ethical standards • Build capacity in the activist/community sector for ethical deliberation and debate
Microbicide Ethics Consultations Earliest ethics consultation initiated by advocates in 1997 – 55 participants from 23 countries Pre-dated launch of effectiveness studies of novel microbicides in developing countries Ethics working group of HPTN Global Campaign ethics consultations held in March and October of 2004
2003 – 2005 Our Ethics Work Expands • Consultation on HIV treatment in the context of prevention trials (in collaboration with IAVI) • Global Consultation on Ethical Issues in the Clinical Testing of Microbicides • (64 people from 12 countries) • GCM Steering Committee drafted Consensus Statement on SOC • Ethics training for advocates and community members
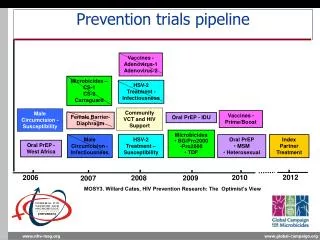
What prevention interventions are being tested? • Microbicides • Substances that can reduce the transmission of HIV and other STD pathogens when applied vaginally and, possibly, rectally. • HIV Vaccines • Oral Tenofovir • Once a day prophylactic pill • Male Circumcision • Acyclovir .
Special Challenges of HIV Prevention Trials • Complex clinical trial design • Healthy individuals -- yet at “high risk” • Often involved marginalized or stigmatized populations (sex workers, IDU, MSM) • Stigma associated with HIV and sexual activity • Transnational research collaborations
Primary difference with Treatment Trials • Little Pharma involvement– all funded through governments and foundations • Less incentive for people to participate because they are not sick • No surrogate markers – only relevant outcome is actual HIV infection • Can’t rely on changes in viral load or CD4 count • In treatment trials, people come to you • “affected community is clear”
Extra Challenges of Microbicide Trials • New, unfamiliar type of product • Can’t actually know whether drug is used • Touches upon sensitive issues – sex, power, gender • Enrolls women only, so pregnancy is on-going threat to validity • Investigators are mostly Gynecologists without experience in HIV treatment
Microbicides: What do we need to know? • Are they Safe for all potential users and uses: • Sexually active women, pregnant women, HIV-positive women, men, adolescents • Vaginal and rectal applications • Effective for key groups of users • Affects Fertility? Contraceptive? or not • Compatible with condoms and other barriers
5 products 2 products 9 products 10-20 products Laboratory & Animal Testing 2-6 Years Phase 1 (safety) 1 to 6 Months Phase 2 (safety) Up to 2 Years Phase 3 (efficacy) 2 to 4 Years 200-400 people 3,000-10,000 people 25 – 40 people Simultaneous studies: HIV+, penile & rectal 10 or more years The Product Pipeline
Basic Design for Microbicide Effectiveness Trials (Phase III) 1 Informed Consent Enrollment visit: STD treatment Condoms, STD treatment + product Recruit Randomize 2 Informed Consent Condoms, STD treatment + placebo Screening visit: HIV, PAP, pregnancy
Family Planning Condom plus placebo INFORMED CONSENT to be SCREENED INFORMED CONSENT to be ENROLL Recruitment: Participant receives information about the trial. Screening Visit 1: Education about the trial, HIV and pregnancy test, STD tests and treatment, baseline data collected Screening Visit 2: Results of tests, counseling, reinforce education about trial Raqndomization: Participant assigned by chance to a group. Condom plus experimental gel Experience of phase III participant
Avoiding Exploitation • “Are trial participants guinea pigs?” • Based in historic experience of exploitation of vulnerable populations for research • Why are you doing the trial here? • Need to “unpack” the issues and implications around this statement.
Unpacking Concerns • Who is conducting the research? • Who benefits from the research? • Why do the research among this population/ community? • What will the research contribute? • Are trial participants “expendable?” • Who makes decisions about this research?
Why are most of the phase III trials taking place in Africa and Asia? • Microbicide trials require large numbers of women at risk of vaginally transmitted HIV • High incidence • Relatively stable (non-transient population) • Little or no injection drug use • Anal sex relatively uncommon • Most populations of women in the US or Europe with high HIV incidence also use IV drugs
Sample Size Calculations Effectiveness Annual HIV Sero-Incidence 1% 2% 3% 4% 5% 20% 110266 54638 36094 26824 21259 30% 46315 22965 15181 11289 8955 40% 24539 12176 8056 5995 4760 50% 14736 7320 4847 3609 2868 60% 9560 4753 3612 2351 1868 70% 6529 3249 2158 1612 1282 80% 4621 2304 1532 1144 913 90% 3353 1673 1115 835 666 Notes: Significance level = .05, power = 90%, test statistics and log rank test, two-tailed, equal size groups. Assumes 15 percent loss to follow-up. Figures prepared by Charlotte Ellertson and Kelly Blanchard using nQuery (version 1.0) survival analysis option.
Additional Criteria for phase III trials • Research infrastructure exists or can be strengthened • Trained investigators • Lab facilities for STD and HIV diagnosis • HIV testing and counseling facilities • Referral services for people who test HIV+ at screening • Research findings should be relevant to and potentially benefit the individuals and communities that participate
Will participating in trials increase women’s risk of HIV? • Generally, no... • Women will become infected during the trial but not because of the trial • Women in both arms should have lower HIV prevalence than women in the general community ` Condoms only Condoms + placebo gel Risk Condoms + microbicide (if it works) Before trial During Trial
But questions remain…. • What is the appropriate balance of risks and benefits in HIV prevention research? • Is it possible to conduct ethical research in a fundamentally unjust world? • Whose voices should be part of the decision process?
clinical trial sites Antwerp, Belgium London, UK New York, USA Cincinnati, USA Washington, USA Providence, USA Philadelphia, USA Los Angeles, USA Baltimore, USA Norfolk, USA Houston, USA Ghana Birmingham, USA Côte d’Ivoire India Chiang Rai,Thailand Miami, USA Dominican Republic Nigeria Uganda Yaoundé, Cameroon Tanzania Malawi Zimbabwe Zambia Brazil Botswana South Africa Alliance for Microbicide Development