Download
1 / 23
240 likes | 738 Vues
Lymphocyte Proliferation Response in Soy Allergy. J. Andrew Bird, M.D. Fellow, Pediatric Allergy and Immunology Texas Children’s Hospital Baylor College of Medicine Houston, Texas. Background. Soy is listed as one of the 8 major food allergens. 1

E N D
Lymphocyte Proliferation Response in Soy Allergy J. Andrew Bird, M.D. Fellow, Pediatric Allergy and Immunology Texas Children’s Hospital Baylor College of Medicine Houston, Texas
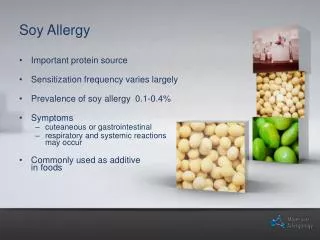
Background • Soy is listed as one of the 8 major food allergens.1 • Soy can be found in many foods including mayonnaise, salad dressings, commercially processed hamburger patties, candies, and pasta. 1 Food and Agriculture Orgainzation of the United Nations (1995) Report of the FAO Technical consultation on Food Allergies 1995. Rome, Italy.
Prevalence of Soy Allergy in High Risk Infants • Cantani meta-analysis, 19972 • Looked at 17 different studies regarding soy protein formula allergy in high risk infants. • High-risk infants – based on atopic history status of parents and/or siblings • Soy allergy occurred in 3 – 4 % of subjects vs. 25% for cow’s milk • No occurrences of anaphylaxis reported. Mostly GI related or AD symptoms. 2Cantani, A. and Lucenti, P. (1997). Natural history of soy allergy and/or intolerance in children, and clinical use of soy-protein formulas. Pediatr. Allergy Immunol. 8:59-74.
Prevalence of soy in atopic individuals • Patients with atopic symptoms • Magnolfi et al. – 704 atopic children – 21% soy positive by SPT and 1.3% soy positive by DBPCFC3 • Bruno et al. – 505 atopic children – 6% soy positive by SPT and 1.8% soy positive by DBPCFC4 • Burks et al. – 13% soy positive by SPT and 1.8% soy positive by DBPCFC in 165 patients5 3Magnolfi, C et al. Soy allergy in atopic children. Ann. Allergy Asthma Immunol. 77:197-201. 4Bruno G, et al. Soy allergy is not common in atopic children: a multicenter study. Pedatr. Allergy Immunol. 8:190-193. 5Burks et al. Atopic dermatitis and food hypersensitivity reactions. J. Pediatr. 132:132-136.
Limitations for defining soy prevalence • Overall – high rate of false-positive results when SPT and RAST are used to diagnose symptomatic soy food allergy. • Need for DBCPFC to clearly define allergy
Advances in Food Allergy • Skin prick test – Hill (2004)6 - 100% PPV for milk, egg, and peanut • No determination for soy. • RAST – Sampson (2001)7 - 90% and 95% PPV for egg, peanut, cow’s milk, and fish. • RAST PPV for soy not defined to 90 or 95% PPV • DBPCFC still gold standard for diagnosis of soy allergy 6Hill, D et al. The diagnostic value of skin prick testing in children with food allergy. Pediatric Allergy and Immunology 2004: 15; 435-441. 7 Sampson H. Utility fo food –specific IgE concentrations in predicting symptomatci food allergy. JACI, May 2001. Vol 107, No 5, pp 891 – 896.
Lymphocyte Proliferation Responses • T-cell sensitization has been demonstrated to play a role in both IgE- and non-IgE-mediated food allergy • Roehr et al. (2001) and Niggemann et al., (2000) - Atopy patch tests used in conjunction with other diagnostic modalities predictive of reaction. • LPR to cow’s milk – conflicting results with studies – felt there is no significant LPR (Hoffman, Ho, Sampson, 1997).
Lymphocyte Proliferation Responses • LPR to egg - specifically ovalbumin • more marked and prolonged in egg allergic patients as compared to non-allergic controls (Ng et al., 2002) • No studies published regarding LPR to soy.
Study Aim • To evaluate whether soy extract can cause in vitro T cell stimulation in non-allergic and/or known soy allergic controls • To identify if an LPR threshold exists between non-allergic and known soy allergic individuals.
Design • Selection of patients based on review of patient database for those seen with diagnoses of anaphylaxis or food allergy. • Chart review will further select those patients with a history of soy allergy based on history of repeated clinical reactivity and/or soy-specific IgE testing. • Symptoms to include eczema, eye, nasal, respiratory or GI IgE-mediated symptoms.
Design • Subjects • 70 patients • 35 soy allergic volunteers • 35 controls • Age-matched ranges of 1 to 12 y/o and > 12 y/o. • Controls must tolerate soy orally by history and have soy-specific IgE as measured by CAP RAST < 0.35 kU/ml. • Statistical Analysis • T-test to compare LPR tests between matched groups
Design • Inclusion criteria • Clinical reactivity upon soy ingestion with detectable soy-specific IgE>0.35 kU/ml. • Anaphylaxis • No anaphylaxis • Includes eczema, eye, nasal, respiratory or GI IgE-mediated symptoms • 1 to 12 y/o vs. > 12 y/o
Design • Exclusion criteria • Excluded if they: • tolerate soy orally • are without clinical reactivity • and have no detectable soy-specific IgE. • Control subjects will be excluded if they: • have clinical reactivity upon soy ingestion • or soy-specific IgE>0.35 kU/ml.
Patients at TCH 38 30 17 14 Total: 41 patients with soy allergy
Patient Recruitment • Fliers sent to local allergists • Over 120 mail-outs with recruitment poster. • Announcements at local allergy society meetings. • Plan on follow-up phone calls.
Procedure • First visit • All subjects will have blood drawn for LPR. • PBMCs will be isolated from whole blood via Ficoll separation. • LPR performed with soy extract at 50,125,250, and 500 mg/mL. • Concomitant studies will be performed using Candida 1:200 (positive control) and RPMI (negative control) • Each well will be pulsed with 3H-thymidine and harvested 18 hours later. • CAP RAST to soy will be obtained if not obtained in past year.
Procedure • First visit, cont. • All patients without anaphylaxis will have skin prick tests and atopy patch tests placed. • SPT performed using soybean reagent (Greer laboratories, 1:20 concentration) and histamine and saline controls • APT performed using 50 microliters of soy milk on filter paper and applying to unaffected skin on the patient’s back by using 12-mm aluminum cups on adhesive tape (Finn chambers on Scanpor). • Occlusion time will be 48 hours and results will be read 24 hours after removal for the final evaluation of the test. • Eczema assessment with SCORAD.
Potential Impact • Determine feasibility of an alternative/adjunctive diagnostic procedure for soy allergy that could yield applicable results within 2 to 3 years. • Potentially eliminate the need for DBPCFC and better define the pathogenesis behind manifestations of soy allergy.
Current Status • Recently received IRB approval. • Patient recruitment • Fliers sent to allergy private practice groups. • Calling within TCH Allergy/Immunology cohort.
Special thanks to Dr. Carla Davis, Dr. Celine Hanson, Dr. Kim Shanks, Dr. Duyen Nguyen, and Dr. Christy Nance • Questions????