Download
1 / 29
310 likes | 1.05k Vues
Chronic Kidney Disease: Progression Modifying Therapies Chapter 46. Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies. Abbreviations. Key Concepts. Chronic Kidney Disease (CKD) US Prevalence ~19 million

E N D
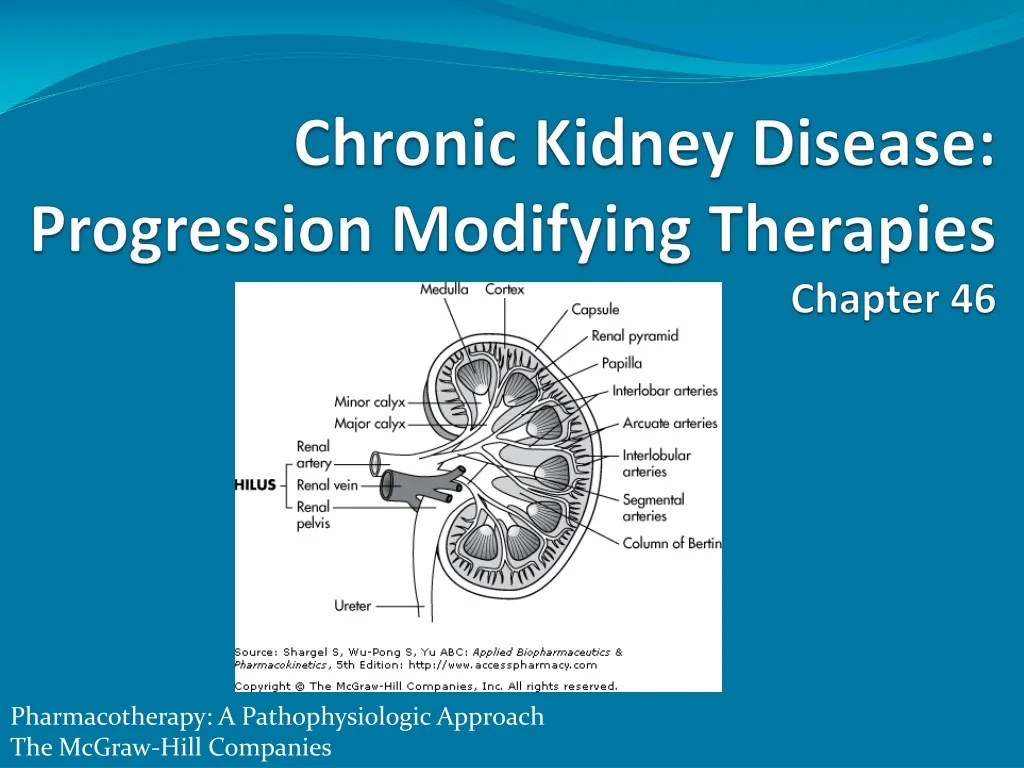
Chronic Kidney Disease: Progression Modifying Therapies Chapter 46 Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies
Key Concepts • Chronic Kidney Disease (CKD) US Prevalence • ~19 million • The Kidney Disease Outcomes Quality Initiative (K/DOQI) • CKD risk factor categories • susceptibility factors • initiation factors • progression factors
Key Concepts • Mechanisms of CKD progression • reduction in kidney mass • glomerular hypertension • intratubular proteinuria • 5 CKD stages based on • structural damage • renal function
Key Concepts • Serum creatinine (SCr): • unreliable marker of kidney function in select patients • elderly • malnourished • children • estimate GFR • used to evaluate rate of disease progression
Key Concepts • Stage 5 CKD symptoms: • asterixis • pruritus • dysgeusia • nausea, vomiting • anorexia, weight loss • susceptibility to bleeding • Signs/symptoms of uremia foundational to decision to implement kidney replacement therapy
Key Concepts • Titrate ACEI/ARB to maximal suppression of urinary albumin excretion for DM patients with persistent microalbuminuria despite intensive insulin therapy • even without HTN • ACEIs/ARBs: key pharmacologic treatments • hemodynamic & BP reduction effects limit kidney disease progression
Key Concepts • Supportive therapies may slow CKD progression • dietary protein restriction • lipid-lowering medications • smoking cessation • anemia management • Limit progression with hyperglycemia & HTN treatment
Epidemiology • Worldwide public health problem: “silent epidemic “ • CKD affects ~5% of adult US population • CKD defined as SCr > 1.2 to 1.5 mg/dL • The Third National Health And Nutritional Examination Survey (NHANES III) • nationally representative sample of US adult population • > 10.9 million people have SCr> 1.5 mg/dL • CKD prevalence ~10.9% of US population age > 20 yrs (19 million) if microalbuminuria & proteinuria included Levey AS, Coresh J, Balk E, et al. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann Intern Med 2003;139:137–147. Jones CA, McQuillan GM, Kusek JW, et al. Serum creatinine levels in the U.S. population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 1998;32:992–999.
Etiology • Susceptibility factors: • advanced age • low income or education • racial/ethnic minority status • reduced kidney mass • low birth weight • family history • Useful for identifying populations at high risk for CKD
Etiology • Initiation factors: • result in direct kidney damage • modifiable by pharmacologic therapy • DM, HTN, autoimmune diseases, polycystic kidney disease, systemic infections, urinary tract infections, urinary stones, lower urinary tract obstructions, drug toxicity • Most common causes of CKD in the US: • diabetes mellitus • HTN • glomerular diseases
Etiology • Progression factors: • associated with further kidney damage • evident as increased decline in kidney function in patients who already have kidney damage • proteinuria, elevated BP, smoking • Predictors of progressive CKD: • persistence of underlying initiation factors • DM • HTN • glomerulonephritis • polycystic kidney disease
The Kidney • 2 million nephrons • filter • reabsorb • excrete solutes • excrete water • Primary regulator • Na+ & H2O balance • acid–base homeostasis • Hormone production necessary for RBC synthesis & Ca2+ homeostasis
Pathophysiology • Heterogeneous causes • diabetic nephropathy: glomerularmesangial expansion • hypertensive nephrosclerosis: kidney's arterioles have arteriolar hyalinosis; renal cysts present in polycystic kidney disease • initial structural damage may depend on the 1˚ disease • Progressive nephropathies result in irreversible renal parenchymal damage & ESRD • Key pathway elements • loss of nephron mass • glomerular capillary hypertension • proteinuria
Pathophysiology • Initiation factor exposure • remaining nephrons hypertrophy to compensate for loss of nephron mass and renal function • compensatory hypertrophy may be adaptive • hypertrophy may lead to intraglomerular hypertension • possibly mediated by angiotensin II
Kidney Disease/Injury • acute renal failure: • rapid loss of kidney function • hours to weeks • 50% increase in SCr (> 0.5 g/dL) • chronic kidney disease: • also called chronic renal insufficiency, progressive kidney disease • progressive loss of function • months to years • gradual replacement of normal kidney architecture with interstitial fibrosis
Kidney Disease Classification • National Kidney Foundation's (NKF) Kidney Dialysis Outcomes & Quality Initiative (K/DOQI) CKD classification system (stages 1 to 5) • Categories based on structural kidney damage &/or functional changes in GFR for > 3 months • stage 1: mild structural changes evidenced by microalbuminuria with "normal" kidney function • stage 5: analogous to end stage renal disease: dialysis or kidney transplantation may be necessary • increasing number: more advanced stage of disease • SCr: inaccurate index of GFR
Kidney Disease • Normal adult kidney function • GFR ~120 mL/min/1.73 m2 • Can diagnose CKD when GFR > 90 mL/min/1.73 m2 based on: • proteinuria • hematuria • evidence of structural damage from kidney biopsy
CKD Stages a Glomerular filtration rate (mL/min/1.73 m2) b CKD can be present with normal/near normal GFR if other markers of kidney disease are present c Based on elevated albumin to creatinine ratio dincludes patients on dialysis DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Presentation/Diagnosis • Development & progression may be insidious • CKD diagnosis • measure SCr, estimate GFR • assess urine for protein &/or albumin • CKD stages 3, 4, 5 require additional workup • anemia • CV disease • metabolic bone disease • malnutrition • fluid & electrolyte disorders
CKD Risk Factors DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Diabetes • Not all individuals with diabetic nephropathy progress to stage 5 CKD; however, high lifetime risk • Multiple Risk Factor Intervention Trial (MRFIT) • prospective study • > 300,000 individuals screened • ~3% of DM patients develop stage 5 CKD • DM subjects: 12-fold greater RR of stage 5 CKD • increased risk of nondiabetic CKD causes • suggests underlying genetic susceptibility Brancati FL, Whelton PK, Randall BL, Neaton JD, Stamler J, Klag MJ. Risk of end-stage renal disease in diabetes mellitus: A prospective cohort study of men screened for MRFIT. Multiple Risk Factor Intervention Trial. JAMA 1997;278:2069–2074.
Diabetes & CKD • Type 1 DM patients: 40% lifetime risk of developing CKD • Type 2 DM patients: 50% lifetime riskof developing CKD • Greater prevalence of type 2 DM compared to type 1 • 10:1 ratio in most countries • majority of CKD due to DM among type 2 DM patients Hasslacher C, Ritz E, Wahl P, Michael C. Similar risks of nephropathy in patients with type I or type II diabetes mellitus. Nephrol Dial Transplant 1989;4:859–863.
Hypertension • Increases CKD risk • Exact role as cause/consequence debated • Kidney has a role in HTN development/modulation • Generally develops concomitantly with progressive kidney disease • Early HTN treatment to aggressive goals slows CKD progression
Hypertension • Multiple Risk Factor Intervention Trial • 1˚ prevention • evaluated effect of an intervention on CHD mortality • 16 year follow-up • lifetime risk of stage 5 CKD for patients with HTN: 5.6% • risk varied dramatically by BP • 0.33% SBP 140 to 150 mm Hg &/or DBP 90 to 100 mm Hg • 4.5% for SBP > 180 mm Hg or DBP > 110 mm Hg Klag MJ, Whelton PK, Randall BL, et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996;334:13–18.
Hypertension • Elevated BP increases risk for developing CKD • Prospective study (n=316,675) managed care patients • increased stage 5 CKD risk in patients with elevated baseline BP • odds ratio for CKD development: • 2.0 (95% confidence interval [CI] 1.6 to 2.5) for SBP 120 to 129 mm Hg & DBP 80 to 84 mm Hg diastolic • 4.3 (95% CI 2.6 to 6.9) for SBP > 210 mm Hg or DBP >120 mm Hg compared to BP SBP < 120 and DBP < 80 mm Hg Perneger TV, Nieto FJ, Whelton PK, Klag MJ, Comstock GW, Szklo M. A prospective study of blood pressure and serum creatinine. Results from the "Clue" Study and the ARIC Study. JAMA 1993;269:488–493. Hsu CY, McCulloch CE, Darbinian J, Go AS, Iribarren C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch Intern Med 2005;165:923–928.
Glomerulonephritis • Glomerular diseases: initiation factors with variable epidemiology, pathophysiology • Goodpasture's disease or Wegener's granulomatosus may progress rapidly to stage 5; cause ARF • Immunoglobulin (Ig) A nephropathy, membranous nephropathy, focal segmental glomerulosclerosis, lupus nephritis, & others more indolent cause of CKD • chronic glomerular diseases progress at variable rates • loss of GFR 1.4 to 9.5 mL/min/year
Interesting, right? This is just a sneak preview of the full presentation. We hope you like it! To see the rest of it, just click here to view it in full on PowerShow.com. Then, if you’d like, you can also log in to PowerShow.com to download the entire presentation for free.




















