Download
1 / 74
740 likes | 931 Vues
Skin Conditions in sports. Introduction…. The skin, the largest organ of the human body, is often involved in sports injuries, which range from simple wounds to a variety of bacterial, fungal, and viral infections

E N D
Introduction… • The skin, the largest organ of the human body, is often involved in sports injuries, which range from simple wounds to a variety of bacterial, fungal, and viral infections • This chapter discusses the basic anatomy of the skin and describes the categories of wounds and their care • Obviously, the risk of the human immunodeficiency virus (HIV) and hepatitis B infection must be considered whenever a potential exposure to blood exists • This chapter presents the latest guidelines available for the prevention of accidental exposure to human blood
Introduction… • Next, the chapter covers skin conditions related to excessive exposure to ultraviolet light, with an emphasis on prevention and safety precautions • Any number of microorganisms, ranging from minute viruses and bacteria to relatively large fungi, can produce skin infections • Information in this chapter introduces the reader to the common types of skin infections in sports, with helpful descriptions of signs and symptoms as well as recommended treatment and prevention protocols
Introductions… • The National Collegiate Athletic Association (NCCA) guidelines on wrestling and skin infections are included, along with a listing of conditions to be considered • This section also covers a related group of skin conditions resulting from allergic reactions to plant toxins and other materials
Introduction… • The skin, or common integument, represents the largest organ of the human body • Two major layers of tissues, the epidermis and dermis, combine to form this complex organ, which has a total surface area of 3,000 square inches on the average adult (American Academy of Orthopaedic Surgeons [AAOS], 1991)
Introduction… • Located immediately beneath the skin is a layer of subcutaneous fat that helps to insulate the body from the external environment
Introduction… • Skin thickness varies regionally on the body: • Thicker skin covers areas subject to pressure • Such as the soles of the feet and palms of the hands • Thinner skin covers areas where joint mobility is essential • The skin serves a variety of purposes, not the least of which is protecting the body from the environment • It is also essential for controlling fluid balance within the body, protecting the body from disease organisms, and regulating body temperature
Introduction… • Furthermore, it houses nerves of sensation that register touch, temperature, and pressure • In addition, specialized cells within the skin produce vitamin D (AAOS, 1991)
Introduction… • The skin can be damaged in a variety of ways during participation in sports. • External trauma can cause wounds, and damage can result from exposure to ultraviolet rays (sunlight) as well as burning or freezing temperatures. • Skin infections can arise from a variety of organisms, including viruses, bacteria, and fungi. • In addition, allergies can also affect the skin; these may be related to contact with plants or clothing and equipment that contain chemicals to which the athlete is sensitive
Wounds… • Sports injuries can cause many types of wounds, ranging from abrasions (scrapes, burns, strawberry) to lacerations (cuts and gashes), all of which may result in infection as well as cosmetic complications (American Medical Association [AMA], 1968).
Wounds… • The primary goals of initial wound care are control of bleeding followed by prevention of infection through cleaning and bandaging
Wounds… • A primary concern when rendering first aid care for any wound is to avoid contact with the whole blood that may transmit infectious organisms such as the human immunodeficiency virus (HIV) or hepatitis B virus (HBV). • The majority of wounds seen in sports are abrasions caused by rubbing, scraping, and burning; lacerations produced by a blunt object tearing the skin; and incisions caused by sharp objects.
Wounds… • A special type of abrasion, known as turf burn, has been associated with playing surfaces in stadiums made of artificial turf • Turf burns are the result of falls sustained on artificial turf that produce friction and heat
Treatment… • Treatment of wounds in sports can be considered as a two-phase process • Initial first aid care is designed to control bleeding and guard the area from further injury • This is followed later with ongoing protection of the area so that return to participation is possible while healing takes place
Treatment… • An important aspect of wound care is protection of fellow athletes, coaches, and other personnel from exposure to whole blood, which can result in the transmission of HIV and HBV organisms. • Risk of exposure involves not only the wound itself, but also blood-soaked clothing and any blood that may be on playing surfaces.
Treatment… • Initial treatment of wounds follows first aid protocol described by the National Safety Council (1993). These are its guidelines: • Before rendering first aid, precautions should be taken against the possible transmission of HIV and HBV. Wear latex gloves and dispose of all waste in a storage container for biohazardous material. • Remove clothing and/or equipment covering the wound. • Control bleeding with direct pressure over the wound site by applying some type of sterile dressing. • If dressing becomes soaked with blood, add more dressings on top. Do not remove blood soaked dressings.
Treatment… • although rare in sports, severe bleeding may not respond to direct pressure. In such cases, combine direct pressure with elevation. • Increased hemorrhage control can be achieved via the application of a pressure bandage to a point over either the brachial or femoral arteries, depending on location of the wound. Once pressure is applied to either of these points, it should not be released until the athlete is under the care of a physician • Tourniquets should be applied only as a last resort; they are rarely needed in first aid for sports-related wounds. • All materials used to treat the wound– gauze pads, towels, and paper towels—should be stored for later disposal identified as containing biohazardous materials.
Treatment… • At the time of initial first aid, a decision must be made about whether the athlete will be allowed to return to participation. • Obviously, the health and safety of the athlete must be the first priority; however, the majority of sports-related wounds are not life-threatening occurrences. • Another consideration is protection of other participants, coaches, and personnel from exposure to whole blood from any wound • In sports such as wrestling, tackle football, and basketball, wounds must be dealt with in such a way to protect other athletes and the coaching staff from incidental exposure
Treatment… • Although research indicates the risk of transmission of HIV and exist (Calabrese, Haupt, & Hartman, 1993) • Once the initial bleeding is arrested, a commercially made dressing should be applied to the wound and held in place with an adhesive bandage. • Small wounds are usually treatable by simply applying a bandage; larger wounds, such as a strawberry on the thigh or arm may require a large sterile gauze pad that is held in place with adhesive tape. • Such bandages should be rechecked periodically during participation to ensure that they remain in proper position and bleeding has not resumed.
Treatment… • Lacerations and incisions, particularly those to the scalp or face, merit special attention because of their potential cosmetic impact. • Such wounds should be referred to a physician for further evaluation and possible stitches. • As a general rule, any wound going below the dermal layer that is more than a centimeter in length—especially if it is on the face—should be seen by a physician for evaluation.
Treatment… • The National Safety Council (1993) provides the following guidelines for cleaning wounds: • Personnel rendering first aid should protect themselves from direct exposure to whole blood by wearing latex gloves • Wash the wound with a sterile gauze pad saturated with soap and water. Hydrogen peroxide (3% solution) may be used to bubble away blood clots and related debris. This is especially helpful when treating abrasions containing significant amounts of dirt and other foreign material.
Treatment… • Flush the wound with large amounts of water; then dry the area with a sterile gauze pad. • Use isopropyl rubbing alcohol to clean the skin adjacent to the wound site; however, do not apply the alcohol directly to the wound. • Do not apply chemicals such as Mercurochrome, Merthiolate, or iodine to wounds; their effectiveness is minimal, and they may cause an allergic reaction. • Apply a sterile, dry dressing and hold it in place with some type of bandage. For smaller wounds, Band-Aid bandages are effective; for larger wounds, sterile gauze pads held in place with elastic adhesive tape are recommended.
Treatment… • By definition, a dressing is a sterile material, usually gauze, used to cover a wound to control bleeding and prevent contamination. • A bandage is used to hold the dressings in place. Bandages need not be anything more than a folded cravat, strips of cloth, or commercially made elastic adhesive tape that can be directly applied to the skin and holds well even near a moving joint • Severe wounds should be treated for control of bleeding and referred immediately for medical evaluation.
HIV/HBV and the Athlete • Although the majority of national focus regarding these two viral infections has focused primarily on HIV, HBV has been on the increase as well. • It is estimated that 300,000 new HBV infections occur each year. • In 1981, the first diagnosed case of acquired immune deficiency syndrome (AIDS) was reported. • In 1986 there were approximately 2,000 people infected with HIV in the US; recent data from the Centers of Disease Control and Prevention (CDC) indicate an estimated 1,106,400 diagnosed cases of HIV in the US through 2006 (CDC, 2008).
HIV/HBV and the Athlete • Virtually anyone who is sexually active, including athletes, is at risk of contacting HIV. • Athletes who inject anabolic steroids may also be at risk of infection, especially when sharing needles (Calabrese, 1989). • The virus is spread primarily through blood-to-blood exposure, which can easily occur when sharing needles during intravenous drug use. • HBV is a bloodborne pathogen and is most easily spread via blood-to-blood contact with an infected person. • Both HIV and HBV are carried within the blood of infected persons; therefore, any time such individuals sustain a bleeding wound, the possibility of transmission exists. • This is especially true if another athlete who also has an open wound comes into contact with the blood of an infected person.
HIV/HBV and the Athlete • Although the chance of such an occurrence may be remote, some precautions are necessary, especially in sports in which external bleeding is likely. • The Occupational Safety and Health Administration (OSHA) developed a comprehensive set of guidelines for health care workers regarding prevention of exposure to HIV and HBV.
HIV/HBV and the Athlete • Coaches and athletes are routinely exposed to blood-contaminated towels, water bottles, playing surfaces, and blood-soaked bandaging materials. • As a result, the prudent coach should make every effort to follow the basic preventive guidelines for HIV and HVB transmission. • Athletes participating in wrestling, tackle football, and boxing frequently sustain bleeding wounds. • It is advised that coaches and officials remove players from participation when excessive bleeding is evident.
Ultraviolet Light-related skin problems… • Outdoor sports played during the summer can result in exposure of large areas of the body to harmful rays of the sun • Typically, summer sportswear does not cover the arms and legs; in some sports, such as swimming and diving, major portions of the skin are unprotected • Medical evidence is substantial that even minor sunburn can be harmful to the skin; it may lead to serious, even lethal, complications such as skin-related carcinomas and melanomas (Reichel & Laub, 1992).
Ultraviolet Light-related skin problems… • Two different wavelengths of ultraviolet light are involved in the sunburn process: • Ultraviolet A (UVA) • Ultraviolet B (UVB) • UVB is a shorter wavelength than UVA and seems more related to the development of skin problems (Rustad, 1992)
Ultraviolet Light-related skin problems… • It is well known that some individuals are at a higher risk for damage from sunlight exposure, including those with lighter skin, red hair, and freckles (Reichel & Laub, 1992) • Exposure to sunlight at any time of the day can result in sunburn; however, the most dangerous times are between 10:00 am and 2:00 pm
Ultraviolet Light-related skin problems… • Sunburn has two clinical phases. • The first, known as the immediate erythema phase, involves reddening of the skin, which occurs during exposure to sunlight • the second phase, called the delayed erythema phase, normally develops within a few hours of exposure and peaks at 24 hours (Reichel & Laub, 1992) • Although most cases of sunburn result in mild discomfort, with symptoms diminishing within a day or two, more severe cases can include the formation of blisters associated with chills and GI distress
Ultraviolet Light-related skin problems… • The primary concern should be on protection of the exposed skin when an athlete is participating in outdoor sports • Certain body areas may require special protection with a commercially prepared sunscreen—particularly the outer ear, nose, lips, back of neck, forehead, forearms and hands
Ultraviolet Light-related skin problems… • Though many sunscreen products are available, athletes should use only those rated with at least a sun protection factor (SPF) of 15 • The SPF rating is derived by determining the sunscreen’s ability to absorb harmful ultraviolet light over time • Thus, athlete’s using a product with an SPF rating of 15 will receive the same amount of ultraviolet light to the skin in 15 hours outdoors as they would have in 1 hour of unprotected exposure
Ultraviolet Light-related skin problems… • TX of sunburn involves application of a commercially made topical anesthetic as well as a skin lotion to help relieve burning and dryness. • In severe cases, medical attention may be warranted, and treatment may include the administration of anti-inflammatory medications
Skin Infections… • A variety of organisms can cause infections of the skin—including fungi, bacteria, and viruses • It should also be remembered that many apparent skin infections can be symptoms of more serious infections and/or allergic conditions including Lyme disease, herpes, or contact dermatitis, and should be referred to a doctor for evaluation
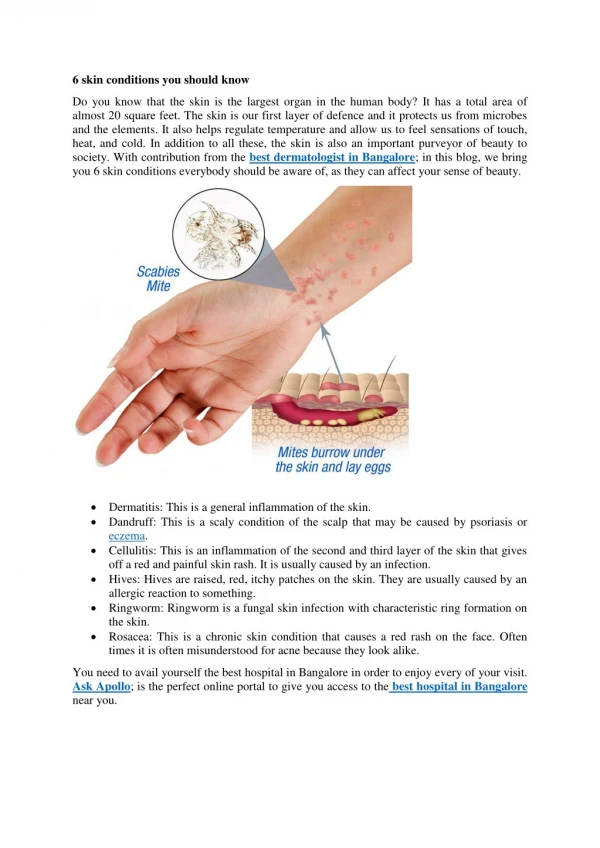
Fungi….tinea (ringworm) • Tinea, commonly known as ringworm, is an infection of the skin caused by a group of fungi • In athletes, the common locations for tinea include the groin region (tineacruris, commonly known as jock itch) and the feet and toes (tineapedis)
Tinea (ringworm) • Tinea infections are common in these body areas because moisture and warmth make them ideal for fungal growth • Tinea can affect other parts of the body as well, including scalp (tineacapitis) and the extremities • Although tinea infections are not serious, if left untreated they may persist and lead to secondary bacterial infections that can be cosmetically displeasing
Tinea (ringworm) • S&S: • Small, superficial, brownish-red, elevated lesions that tend to be circular in shape • When infections involve the toes, lesions may include cracking between the toes associated with oozing and crusting • Itching and pain are associated with both tineapedis and tineacruris • Scaling of the skin over the lesions may also be noted
Tinea (ringworm) • TX: • Vigilant cleaning of the involved areas, followed by drying • Applying an over-the-counter topical treatment such as Tinactin • Apply a moisture-absorbing powder to the area • Wearing clothing made of natural fibers such as cotton
Fungi…..TineaVersicolor (tv) • This particular fungal infection is considered to be the most common warm-weather-related skin problem among teenagers and young adults (Rustad, 1992)
Tineaversicolor (tv) • Gets its name from the symptoms it produces on the skin of the affected person • This infection is characterized by the appearance of lesions that are of a different color than the adjacent, normal skin • It is usually confined to the upper trunk, neck, and upper abdomen (AMA, 1968)
Tineaversicolor (tv) • S&S: • Circular lesions that appear either lighter or darker than adjacent skin • Skin may appear white, in contrast to adjacent unaffected skin, after exposure to sunlight • Lesions normally found on the trunk • TX: • Prescription drugs, either oral or topical • Treatment may require weeks or even months to be effective
Bacterial infections • Bacterial infections of the skin are relatively common in sports that involve close physical contact between participants • Known collectively as pyonderma(pus-producing infection of the skin), these infections are normally caused b y two common bacteria, Staphylococcus Aureus and Streptococcus • The former is related to conditions such as furuncles, carbuncles, and folliculitis • The latter causes impetigo and cellulitis
Bacterial infections… • All of these conditions are characterized by infected, purulent (pus-producing) lesions on the skin • For example, in folliculate the lesions are located as the base of a hair follicle
Bacterial infections… • Furuncles are similar in appearance; however, they form large nodules around the hair follicles and may burst as the infection develops
Bacterial infections… • Impetigo is similar in appearance, but may develop in areas with little or no hair
Bacterial infections… • S&S of furuncles, carbuncles, and folliculitis: • The underlying symptom of all forms of pyoderma is a lesion, regardless of location, that is producing pus • Folliculitis involves lesions located at the base of a hair follicle • Furuncles, commonly called “boils,” are lesions that form large nodules around the base of a hair follicle and may burst as the infection develops • Boils can appear anywhere, but are more common on the arms, armpits, neck and chest, buttocks, and groin • Carbuncles are essentially a collection of boils that together form a weeping, pus-producing lesion typically found around the posterior neck and upper trunk regions
Bacterial infections… • S&S of impetigo and cellulitis • The underlying symptom of all forms of pyoderma is a lesion, regardless of location, that is producing pus • often seen on the face, impetigo presents groups of raised skin lesions that are honey-colored and crusty in appearance • Cellulitis also is a skin infection; however, it affects the deeper layer of skin known as the dermis • The skin will appear red and warmer than adjacent skin and, in addition, will be painful to the touch
Bacterial infections… • Regardless of the specific condition, all pyodermal infections share a common characteristic—the presence of lesions that are obviously infected and associated with drainage and pus formation • Any athlete demonstrating such signs and/or symptoms as described should be removed from participation and referred for medical evaluation
Viral infections… • Two of the more common viral-related skin problems in sports are plantar warts and herpes gladiatorum • As a skin problem, warts are quite common in the general population and occur as the result of infection by a specific group of viruses known collectibely as the human papillomavirus (HPV), of which over 55 specific types have been identified