Download
1 / 12
191 likes | 785 Vues
Pituitary Adenoma. from the anterior pituitary gland ( adenohypophysis ) Microademoas <1cm and Macroadenomas Functional Secreate endocrinologically active compunds at pathologic levels Non Functional Secrete nothing or inactive compunds.

E N D
Pituitary Adenoma • from the anterior pituitary gland (adenohypophysis) • Microademoas <1cm and Macroadenomas • Functional • Secreateendocrinologically active compunds at pathologic levels • Non Functional • Secrete nothing or inactive compunds
Functional tumors are often diagnosed when quite samll due to endocrine dysfunction. The most common syndromes are Cushing’s dissease (ACTH), Forbes- Albright syndrome (prolactin) and acromegaly (GH)
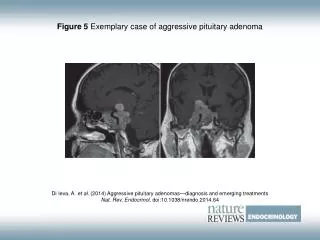
Non functional tumors are diagnosed later as larger lesions causing mass effect such as visual field deficits or panhypopituitarism. Hemorrhage into the pituitaury tumor causes abrupt symptoms of headace, visual disturbances, decreased mental status and endocrine dysfunction (pituitary apoplexy)
Surgical decompression is indicated for symptomatic pituitary tumors to eliminate mass effect or to attempt and endocrine cure. • Prolactin-secreting tumors usually shrink with dopaminergic therapy alone (bromocriptine) • Most pituitary tumors are approached through the nose via the transsphenoidal approach. Minimally invasive endoscopic sinus surgery techniques are being used increasingly.
Chordoma • A chordoma is A rare congenital tumor of the brain developing from the fetal notochord along the axial skeleton. It is usually located in the midline behind the sella , slow growing but highly invasive • Chordomas comprise less than 1% of CNS tumors. As primary intracranial neoplasms, they only constitute 0.2% of all CNS tumors; however, they constitute 2-4% of all primary bone neoplasms.
Chordomas generally occur in 3 locations, which are, in descending order of frequency, the sacrum, intracranially at the clivus, and along the spinal axis.
During development, the notochord is surrounded by the developing vertebral column. In adults, remnants of the notochord are present as the nucleus pulposus of the intervertebral discs. Notochordal remnants that are extradural are most common at the sacrococcygeal region but can be found at any site along the length of the axial skeleton. The distribution of tumors matches the distribution of notochordal remnants.
Chordomas are characterized by slow growth, with local destruction of the bone and extension into the adjacent soft tissue. Very rarely, distant metastases are encountered. These tumors usually have a relatively indolent but prolonged course with multiple local recurrences, and, eventually, they may be responsible for mortality.
clinical presentation is entirely dependent on the location of the chordoma. At the sacrum, common presenting symptoms are back and/or lower extremity pain. About one half of patients with chordomas have autonomic symptoms, particularly rectal dysfunction or urinary incontinence. About one half of patients with chordomas have a palpable sacral mass. • With intracranial tumors, the most common presenting symptoms are diplopia and headache. Neurologic signs also occur in over one half of the patients, primarily as cranial nerve palsies. Palsies of cranial nerve VI and the sensory branch of V are the most common.
Patients with tumors located along lower vertebrae may present with pain, bladder dysfunction, or lower extremity weakness. Patients with tumors located along cervical vertebrae present with hoarseness, dysphagia, and, occasionally, pharyngeal bleeding. Other rare or unique symptoms have been reported but are the exception. The time span from the onset of symptoms to diagnosis averages 10 months.
Medical Therapy • Clinical trials are underway to study the effectiveness of imatinibmesylate in the treatment of chordoma (Casali et al., 2004). Imatinibmesylate is a tyrosine kinase inhibitor targeting several enzymes including platelet-derived growth factor receptor--b (PDGFRB), which can be expressed in chordomas. This drug has been shown to have antitumor activity in chordomas; however, research is ongoing and surgery remains the standard treatment for chordomas. Adjuvant radiation therapy is used in cases where incomplete resection is suspected. Chemotherapy has not been shown to be effective.
Surgical Therapy • The treatment of chordomas depends on the extent and location of the tumor. In general, a more complete removal with wide excision delays the time interval between surgery and eventual recurrence. The natural history and the effectiveness of different kinds of therapy are not well understood in chordomas because of their rare incidence and slow-growing nature. • Radical resections of tumors with clean margins are associated with a longer disease-free interval. If subtotal excision is the only option (generally due to location and proximity to delicate anatomy), the addition of radiation therapy can lengthen the interval to recurrence. In cases in which radiation therapy is utilized without surgical resection, an average of only 50% for 10-year local control is seen for skull-based and cervical spine tumors.