Download
1 / 38
390 likes | 417 Vues
Pituitary disease. Prof Julian Davis Endocrinology Group, School of Biomedicine, University of Manchester Department of Endocrinology, Manchester Royal Infirmary. Hypothalamic-pituitary hormone axes. Hypothal Pituitary hormone - cell Target hormone CRH ACTH - corticotroph cortisol

E N D
Pituitary disease Prof Julian Davis Endocrinology Group, School of Biomedicine, University of Manchester Department of Endocrinology, Manchester Royal Infirmary
Hypothalamic-pituitary hormone axes Hypothal Pituitary hormone - cell Target hormone CRH ACTH - corticotroph cortisol TRH TSH - thyrotroph thyroxine GnRH LH - gonadotroph T, E2 GnRH FSH - gonadotroph inhibin GHRH GH - somatotroph IGF-1 DA Prolactin - lactotroph
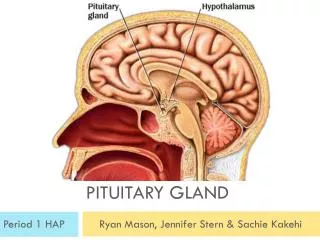
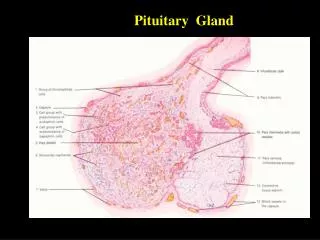
Normal pituitary gland: cell types intermingled ACTH – corticotrophs TSH - thyrotrophs LH, FSH - gonadotrophs GH - somatotrophs Prolactin - lactotrophs Normal pituitary - mixed cell types
Pituitary adenomas Benign, slow-growing Differentiated Local expansion Incidental small tumours common Mass effects - headache, visual loss Hormonal effects - hormone overproduction
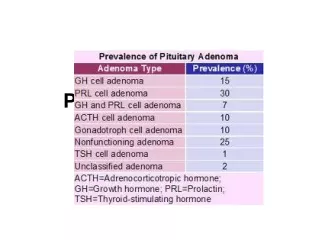
Pituitary tumour types Differentiated tumours containing single pituitary cell types Lactotroph: PRL prolactinoma Somatotroph: GH acromegaly Corticotroph: ACTH Cushing’s disease Gonadotroph: LH, FSH = non-functioning Thyrotroph: TSH
Investigation: pituitary imaging CT scan: axial coronal Lateral skull X-ray
Functioning clonal tumours give endocrine syndromes: PRL excess (prolactinoma) – lactation, amenorrhoea Amenorrhoea Hypogonadism Infertility Galactorrhoea
GH excess: gigantism and acromegaly GH excess Soft tissue and bone growth Tall stature Enlarged face, hands, feet… Metabolic effects: BP, diabetes…
Non-functioning adenomas LH/FSH gonadotroph adenomas: LH or FSH excess rare… usually just α- or ß-subunits, no endocrine effect, hence ‘non-functioning’ → mass effect & hypopituitarism TSH thyrotroph adenomas: TSHoma = very rare cause of thyrotoxicosis
Craniopharyngioma • Rare benign tumours • Remnants of Rathke’s pouch • Solid tissue, cysts, • calcified nodules • Within or above the pituitary
Pituitary tumour pathogenesis • Little definite conclusive evidence • Hormonal environment can predispose to tumours: • oestrogens can induce prolactinoma in rats • D2R knockouts get prolactinoma • NGF overexpression causes prolactinoma • reversible ‘trophic changes’ in pituitary populations may lead to overgrowth of clonal populations? • Intrinsic genetic alterations lead to clonal expansion • gsp mutation can ‘explain’ 40% of Ghomas • no other characteristic mutations identified
Genetic advances – familial pituitary adenomas • MEN-1 • Menin gene 11q13 • Carney Complex • PRKAR1A, 17q22-24; 2nd locus… • McCune-Albright • Gsp oncogene • Familial predisposition syndrome • AIP
Familial adenoma predisposition:discovery of AIP Two extended families, northern Finland Two clusters linked as 1 family by genealogy (generation I from 1700s): 3 cases of acromegaly/gigantism Low penetrance familial adenoma predisposition to PRLoma and GHoma Whole-genome SNP genotyping done on 16 individuals Linkage to 11q13, but no MEN1 mutations AIP gene identified, mutations in cases Vierimaa et al, Science 2006
AIP: Aryl hydrocarbon Interacting Protein • AIP 330 amino-acids • FKBP-homology domain • 3 tetratricopeptide repeats (TPRs) • AIP complexes with aryl hydrocarbon receptor (AHR) and Hsp90 • (AHR = ligand-activated TF) • AIP also binds and impairs function of phosphosdiesterase PDE4A5 and PPAR • Mutations render AIP inactive; • many AIP-assoc adenomas null for AIP protein A. Normal pit; B. AIP-proficient adenoma C-D: acromegaly, AIP Q14X mutation, -ve ICC Georgitsi et al, PNAS 2007
Natural history • Autopsy and scanning data • Autopsy(meta-analysis by Molitch, 1997) • Variable rates: 1-27%, average 11% • males=females • 3 / 1403 are macroadenomas • 46% stained for prolactin • Scanning: • CT: >3mm adenomas in 4-20% (Molitch, 97) • MR: 10 / 100 if 2 reviewers agreed, 25-48 / 100 if one only (Hall, 94)
Natural history • Long-term follow-up • 156 patients followed over 8y (Molitch, 1999) • tumour expansion in 6% • PRL levels stable or fell in 75% • i.e. prolactinomas may be very indolent, may remit, may not need treatment • Worth a trial of withdrawal of drug treatment
Pituitary tumour therapy Surgery Radiotherapy Drug therapy DAs Somatostatin analogues GH antagonists
Transsphenoidal pituitary surgery • Potential for long-term cure and avoidance of DA side-effects • Outcomes poor for PRLomas even in specialist hands - 50-75% long-term endocrine remission for microadenomas
Endoscopic transphenoidal surgery – Manchester experience 2005-2007 125 consecutive patients endoscopic approach single surgeon Comparison of two consecutive 15 month periods 05-0606-07total NF adenomas 22 45 67 Acromegaly 15 7 22 Cushing’s 4 6 10 PRLoma 6 3 9 Cranio 2 2 4 Apoplexy 1 5 6 Macroadenoma 40 66 106 Surgical duration 120 91 101 Hospital stay 7 (3-36) 4 (3-15) 5 Leach et al, Neurosurgery, 2010
Endoscopic surgery - outcomes 61 (49%) had VF deficits … improved in 54 unchanged/worse in 7 Endocrine remission Acro 12/15 6/7 18/22 (82%) Cush. 2/4 5/6 7/10 Hypopit 17% 25% 22% New DI 4% 6% 5% Complications 9% (CSF leak/meningitis, sphenoid sinusitis…) Reoperations 15% (CSF leak, residual tumour) Leach et al, Neurosurgery, 2010
Radiotherapy Prevents tumour regrowth Slow effect Gradual hypopituitarism, Over 10-15 years
Role of radiotherapy • Often used post-op after ‘non-curative’ surgery • Progression-free 15y survival: • 93% after RT • 33% for non-RT
Dopamine agonists • Bromocriptine • introduced 1971 • reduces prolactin in 85-90% • restores gonadal function in 80-90% (women) • significant tumour shrinkage in 80% • mostly in first 3 months, but effect continues • useful shrinkage in 24-48h • Cabergoline, Quinagolide • introduced 1990s • similar PRL response rate • similar adenoma shrinkage rate
Bromocriptine: PRL suppression 55y female PRL 656,000mU/L (NR 100-500) BCR treatment only
Cessation of dopamine agonists: prospective study - Colao et al, (2003) NEJM, 349:2023 • 200 patients 25 non-tumoral • 105 microprolactinoma • 70 macroprolactinoma • -stable on cabergoline, PRL suppressed to normal (25µg/L; 550mU/L) • -small tumour residue, or no residue • Cabergoline withdrawn after 2-5y: recurrence rates… • Non-tumoral hyperprolactinaemia 24% • Microprolactinoma 30% • Macroprolactinoma 36% • possibility of permanent remission, even for macroadenomas • chances better if scan showed no tumour residue • caution for longer term follow-up, but worth trial withdrawal • follow-up study (Clin Endo 2007): PRL and tumour size criteria
Is acromegaly different? SSTRs: receptor targets for medical therapy of GH tumours 5 SSTRs cloned 1990s – wide tissue distribution SSTR-2 and SSTR-5 most highly expressed in pituitary
Somatotroph tumours: modest shrinkage with long-term somatostatin agonists Acromegaly: MRI assessment of primary octreotide therapy 25 patients: 76% showed >25% of tumour shrinkage, after 6 months of treatment. Tumour shrinkage: Mild in 40% - IGF1 normalised in 5/10 Moderate in 24% - IGF1 normalised in 4/6 Remarkable in 12% - IGF1 normalised in 3/3 Figure shows a patient who achieved 75% of tumour shrinkage, but no IGF-I/GH normalization. Jallad, Bronstein et al, Clin Endo 2005
Pituitary tumour shrinkage – response varies Prolactinomas - dramatic shrinkage in 80%+ with dopamine agonists - change in size with oestrogen (more marked in rodent models) Somatotrophinomas - mild-moderate slow shrinkage in ~50% with somatostatin analogues Gonadotroph adenomas – little evidence: eg 7/13 showed 10% shrinkage with long-term dopamine agonist (Lohman, Pituitary, 2001) Review - 5/100 shrinkage with octreotide in 11 studies - 55/199 shrinkage with DAs in 24 studies (Colao, Endo Rel Cancer, 2008) Corticotroph adenomas – no evidence Mechanism – the plastic pituitary, or the plastic lactotroph? Apoptosis in PRLomas? – increased reticulin staining in surgical specimens after DAs Alteration in lactotoph cell size vs cell number?
Clinical databases for measuring and understanding outcomes • UK National Acromegaly Register • Established 1997 • 22 centres • 1920 patients • Outcomes analysis: • Radiotherapy study, 1840 patients • Jenkins et al, JCEM 2006 • Transsphenoidal surgery outcomes, 785 patients • Bates et al, Clin Endo 2007
Acromegaly surgical outcomes ‘safe’ GH 1319 patients underwent TS surgery; 1185 as primary treatment; Interpretable GH data in 785 Interpretable IGF-1 data in 430 Variation in success rates: 20-68% among centres with >10 cases; Overall ‘safe GH’ rate 39% normal IGF-1 Bates et al, Clin Endo, 2007
Surgery for acromegaly: trend for improving results: pre-1985 to 2004 Messages: Increased scrutiny of outcomes by colleagues and patients Improving practice, fewer more specialised pituitary surgeons Stated desirable case-loads (>20 functioning tumours/year)
Summary • Pituitary tumours: benign, indolent, locally destructive. • Cell type of origin determines clinical picture (prolactinoma, acromegaly, Cushing’s, non-functioning etc) • Pituitary adenoma pathogenesis becoming better understood, but still few candidate genes for sporadic adenomas • Natural history of disease more variable than thought – remission occurs • Therapy and outcomes undergoing more scrutiny – role of disease databases