Download
1 / 48
540 likes | 1.49k Vues
Hutchinson-Gilford progeria syndrome (HGPS). PRESENTATION BY DELTA CELL. OUTLINE. BACKGROUND: Etymology and History EPIDEMIOLOGY AETIOPATHOGENESIS CLINICAL FEATURES DIFFERENTIAL DIAGNOSES

E N D
Hutchinson-Gilford progeria syndrome (HGPS) PRESENTATION BY DELTA CELL
OUTLINE • BACKGROUND: Etymology and History • EPIDEMIOLOGY • AETIOPATHOGENESIS • CLINICAL FEATURES • DIFFERENTIAL DIAGNOSES • INVESTIGATIONS • TREATMENT • COMPLICATIONS AND PROGNOSIS • REFERENCES
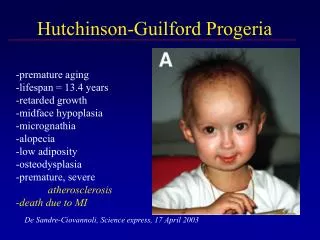
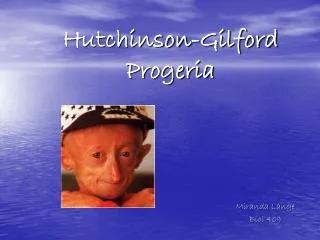
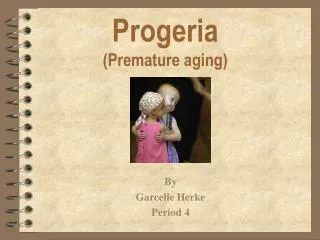
PROGERIA- BACKGROUND Hutchinson-Gilford progeria syndrome (HGPS) is an extremely rare hereditary disease that affects the skin, musculoskeletal system, and vasculature. HGPS is characterized by signs of premature aging. Progeria is a rare genetic condition that produces rapid aging in children.
ETYMOLOGY • The term progeria is derived from the Greek word geras, meaning old age.
HISTORY • In 1886, Hutchinson described the first patient with HGPS, a 6-year-old boy whose overall appearance was that of an old man. In 1887, Gilford described a second patient with similar clinical findings; in 1904, he published a series of photographs depicting the clinical manifestations of progeria at different ages. To date, approximately 100 patients with HGPS have been described in the literature
INTRODUCTION • Significant morbidity and mortality result from accelerated atherosclerosis of the carotid and coronary arteries, leading to premature death during the first or second decade of life. HGPS is considered a segmental aging syndrome, as affected patients do not manifest all of the typical features of aging, such as increased incidence of cancer and neurocognitive decline.
EPIDEMIOLOGY • A study in Norway found the incidence of progeria to be 1 in every 4 million of the population. • Researchers believe that at any given time, there are 200-250 children living with Progeria.
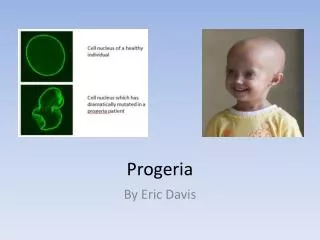
AETIOPATHOGENESIS • The gene responsible for HGPS is called LMNA (pronounced Lamin A). Within this gene there is a change in one element of DNA. This type of gene change is called a point mutation. The LMNA gene makes a protein called Lamin A, which is an important protein for most cells of our bodies. Lamin A is found in the cell nucleus, and helps maintain the integrity of the cell. • Is This Disease Passed Down? • HGPS is not usually passed down in families. The gene change is a chance rare occurrence. Children with other types of "progeroid" syndromes which are not HGPS may have diseases that are passed down in families.
CLINICAL FEATURES • HISTORY Evidence of Hutchinson-Gilford progeria syndrome (HGPS) begins within the first 2 years of life. At birth, infants usually appear healthy, although sclerodermatous skin changes have been noted in some patients. Typically, the onset of the disease occurs at age 6-12 months, when skin changes and alopecia are first noted and when the infant fails to gain weight.
SYMPTOMS • Growth failure during the first year of life • Narrow, shrunken or wrinkled face • Baldness • Loss of eyebrows and eyelashes • Short stature • Large head for size of face (macrocephaly) • Open soft spot (fontanelle) • Small jaw (micrognathia)
SYMPTOMS CONTD • Dry, scaly, thin skin • Limited range of motion • Teeth - delayed or absent formation
CLINICAL FEATURES CONTD • High-pitched voice • Short stature and low weight for height, with prenatal onset of growth failure • Incomplete sexual maturation • Generalized osteoporosis and pathologic fractures • Feeding difficulties • Delayed dentition, anodontia, hypodontia, or crowding of teeth • Low-frequency conductive hearing loss • Hypertension • Prolonged prothrombin time, elevated platelet counts, and elevated serum phosphorus levels
CLINICAL FEATURES CONTD • Emotionally, patients with HGPS share the same feelings as age-matched healthy persons with regard to expressing proper mood and affect. Patients with HGPS are keenly aware of their different appearance and remain reserved in the company of strangers; in the presence of friends, they display affection and good social interaction. • Intelligence is normal.
DIFFERENTIAL DIAGNOSES • SCLEREMA NEONATORUM • OUR OWN DEAR MARASMUS
INVESTIGATIONS • Abnormalities in serum lipid levels are limited to low high-density lipoprotein levels, which are associated with atherosclerotic disease. Serum low-density lipoprotein and total cholesterol levels are normal in patients with Hutchinson-Gilford progeria syndrome (HGPS). • Elevated levels of hyaluronic acid excretion are seen in the urine of patients with HGPS but are not diagnostic. The significance is unknown.
TREATMENT • To date, no effective therapy is available for Hutchinson-Gilford progeria syndrome (HGPS). • Careful monitoring for cardiovascular and cerebrovascular disease is essential. The use of low-dose aspirin is recommended as prophylaxis against cardiovascular and cerebrovascular atherosclerotic disease. • Physical and occupational therapy can help to maintain physical activity and an active lifestyle. The use of hydrotherapy may be particularly effective in improving joint mobility and minimizing symptoms of arthritis.
TREATMENT CONTD • Infants with HGPS may exhibit poor feeding. Provision of adequate nutritional intake may require placement of a gastrostomy tube for supplemental enteral feeding. In older children, the daily consumption of high-energy supplements is recommended, along with careful monitoring of growth and nutrition. • The use of growth hormone has been used to decrease catabolic demands and augment weight gain and linear growth in a small number of patients with progeria.
TREATMENT CONTD • Recently, exposure of cultured HGPS fibroblasts to rapamycin, a macrolide antibiotic that has been shown to regulate aging-related cellular pathways, has been demonstrated to reverse nuclear blebbing, retard cellular senescence, and facilitate degradation of progerin.[24]
TREATMENT CONTD • In vitro studies suggest a possible role for the use of farnesyltransferase inhibitors (FTIs) in HGPS.[25] FTIs appear to promote the release of the mutant prelamin A (preprogerin) from the nuclear membrane, allowing it to be correctly incorporated into the nuclear lamina, thus correcting the structural and functional nuclear defects, although it remains to be determined whether use of FTIs also has an effect on the abnormalities seen in HGPS that result from loss of normal lamin A function. A phase II trial of lonafarnib, an FTI, in progeria is currently ongoing.
TREATMENT CONTD • In vivo studies using FTIs in transgenic mouse models have demonstrated encouraging results with regards to prevention of the cardiovascular complications seen in progeria[26] as well as reversal of the cutaneous manifestations[27] and overall improvement in many of the phenotypic features of progeria, including increased longevity.[28, 29] • Treatment of transgenic mice expressing progerin in the epidermis with FTI-276, a farnesyltransferase inhibitor, or a combination of pravastatin, a lipid-lowering agent, and zoledronic acid, an agent used to increase bone mineral density, has been shown to reverse the morphological nuclear abnormalities that are seen in HGPS.[30]
TREATMENT CONTD • A phase II clinical trial investigating the use of pravastatin, a lipid-lowering agent, zoledronic acid, an agent used to increase bone mineral density, and lonafarnib, an FTI, in patients with progeria is ongoing.
SUPPORT GROUP • Progeria Research Foundation, Inc. --www.progeriaresearch.org • The Progeria Research Foundation, in association with a CLIA-approved diagnostics lab, is pleased to provide a DNA-based, diagnostic test for children suspected of having Hutchinson-Gilford Progeria Syndrome (HGPS).
COMPLICATIONS • Death due to cardiovascular abnormalities occurs in approximately 75% of Hutchinson-Gilford progeria syndrome (HGPS) patients. Other causes of death mentioned in the literature include stroke, marasmus, inanition, seizures, and accidental head trauma. • Heart attack (myocardial infarction) • Stroke
PROGNOSIS • Progeria causes early death. Patients usually only live to their teenage years. However, some patients can live into their early 20s. The cause of death is usually related to the heart or a stroke.
LEON BOTHA • Leon Botha (4 June 1985 – 5 June 2011)[1] was a South African hip hop artist and DJ, as well as one of the world's oldest survivors of progeria. • He died a day after his 26th birthday
REFERENCE • 1. Brown WT. Progeria. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 90. • 2. http://www.ncbi.nlm.nih.gov/pubmed health • 3. http://www.medscape.org