Download
1 / 61
750 likes | 1.65k Vues
Splenic infarcts – gross Coagulative necrosis.

E N D
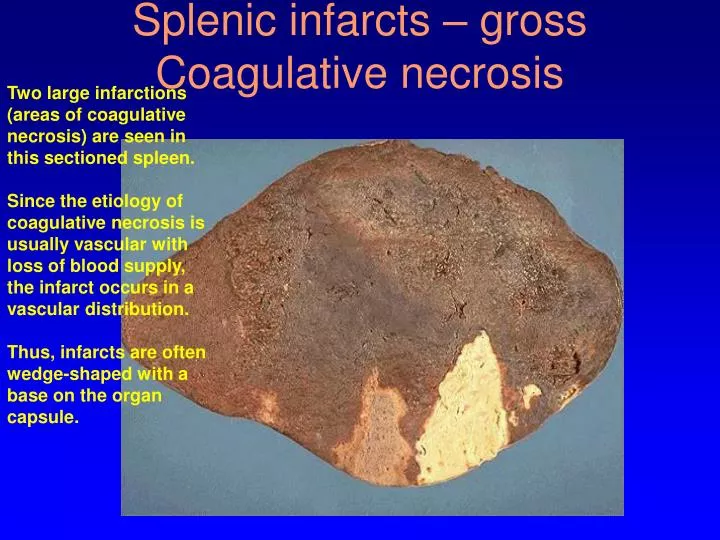
Splenic infarcts – grossCoagulative necrosis Two large infarctions (areas of coagulative necrosis) are seen in this sectioned spleen.Since the etiology of coagulative necrosis is usually vascular with loss of blood supply, the infarct occurs in a vascular distribution. Thus, infarcts are often wedge-shaped with a base on the organ capsule.
Infarcted bowel – grosswet gangrene The small intestine is infarcted. The dark red to grey infarcted bowel contrasts with the pale pink normal bowel at the bottom
Microscopically, the renal cortex has undergone anoxic injury at the left so that the cells appear pale and ghost-like. There is a hemorrhagic zone in the middle where the cells are dying or have not quite died, and then normal renal parenchyma at the far right.This is an example of coagulative necrosis 3 stages of coagulative necrosis (L to R) -- micro
Lung abscesses (liquefactive necrosis) -- gross Extensive acute inflammation may lead to abscess formation, as seen here with rounded abscesses (the purulent material has drained out after sectioning to leave a cavity) in upper lobe and lower lobe
Liver abscess – microliquefactive necrosis The liver shows a small abscess here filled with many neutrophils. This abscess is an example of localized liquefactive necrosis
Liquefactive necrosis -- gross Grossly, the cerebral infarction at the upper left here demonstrates liquefactive necrosis.Eventually, the removal of the dead tissue leaves behind a cavity
Liquefactive necrosis of brain-- micro This is liquefactive necrosis in the brain in a patient who suffered a "stroke" with focal loss of blood supply to a portion of cerebrum.
Organizing liquefactive necrosis with cysts -- gross As this infarct in the brain is organizing and being resolved, the liquefactive necrosis leads to resolution with cystic spaces
Macrophages cleaning liquefactive necrosis -- micro At high magnification, liquefactive necrosis of the brain demonstrates many macrophages at the right which are cleaning up the necrotic cellular debris
Caseous necrosis lungs -- micro Microscopically, caseous necrosis is characterized by acellular pink areas of necrosis, as seen here at the upper right, surrounded by a granulomatous inflammatory process
Fat necrosis pancreas -- micro Microscopically, fat necrosis adjacent to pancreas is seen here. There are some remaining steatocytes at the left which are not necrotic. The necrotic fat cells at the right have vague cellular outlines, have lost their peripheral nuclei, and their cytoplasm has become a pink amorphous mass of necrotic material
Ch. 1, p. 2, Fig. 1-2 Myocyte adaptation
See Ch. 1, p. 3. Fig. 1-3 Physiologic hypertrophy
Muscle atrophy -- micro There are some muscle fibers here that show atrophy.The number of cells is the same as before the atrophy occurred, but the size of some fibers is reduced.This is a response to injury by "downsizing" to conserve the cell
See also Ch. 1, p. 5, Fig. 1-4 Physiologic atrophy
Atrophic testis -- gross The testis at the right has undergone atrophy and is much smaller than the normal testis at the left
See Ch. 1, p. 5, Fig. 1-5 Squamous metaplasia
Ischemia causes cell injury by • Activation of lipases • Activation of proteases • generation of free radicals • initiating inflammation • reducing cellular oxygen
The structures of the cell first affected by hypoxia are • cell membranes • cell nuclei • endoplasmic reticula • Golgi apparatus • Mitochondria
the first manifestation of decreased oxidative phophorylation is characterized by • Cell shrinkage • Decrease glycolysis • Decrease Na+ pump • Increased pH • Increased protein synthesis
Increased cytosolic Ca++ in the cell leads to the activation of proteases, which in turn leads to • Accumulation of lactic acid • Cytoskeletal damage • Decreased ATP production • Decreased phospholipids • Increased protein synthesis
Which of the following is the feature of reversible hypoxic cell injury? • Acute cellular swelling • Apoptotic bodies formation • Denaturation of cellular proteins • Mitochondrial vacuolization • Structural defects of cell membrane
An irreversible injury to the myocardium will have occurred when • Blebs form on cell membrane • Cytoplasmic sodium increases • Glycogen stores are depleted • Intracellular pH diminishes • Nuclei undergo karyorrhexis
A 5 cm cystic area in left parietal lobe of cortex is found at autopsy. This finding is result of? • Caseous necrosis • Coagulative necrosis • Fat necrosis • Fibrinoid necrosis • Liquefactive necrosis
Which of the following is typical pathway for the disseminations of sarcomas? • Direct tumor extension • Hematogenous spread • Lymphatic spread • Seeding of body cavities • Venous spread
Pleomorphism, abnormal nuclear morphology, abnormal mitosis and loss of polarity, are considered hallmarks of • Anaplastic tumors • Benign tumors • Intermediate tumors • Moderately differentiated tumors • Well differentiated tumors