Download
1 / 20
240 likes | 785 Vues
spleen. Dr . Mezjda Ismail Rashaan , consultant surgeon University of sulaymania Faculty of medical sciences School of medicine Kurdistan. Anatomy & physiology. Anatomy:- -origin

E N D
spleen Dr. Mezjda Ismail Rashaan, consultant surgeon University of sulaymania Faculty of medical sciences School of medicine Kurdistan
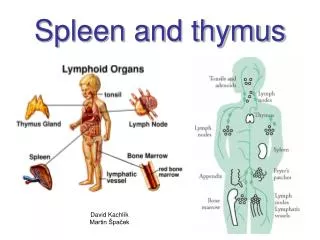
Anatomy & physiology Anatomy:- -origin -location & surface anatomy -its ligaments ; (gastrosplenic, splenocolic, phrenicosplenic, splenorenal) -arterial and venous supply
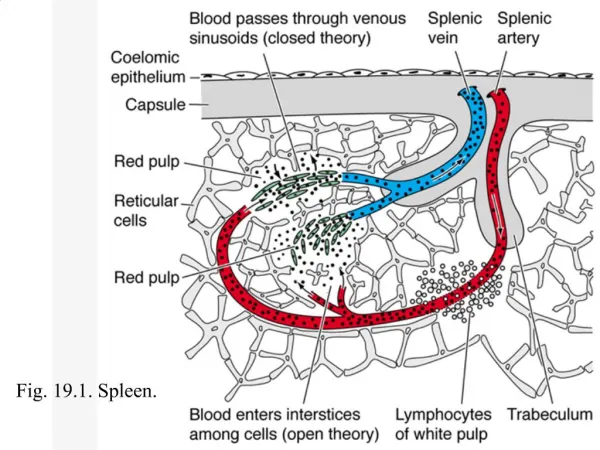
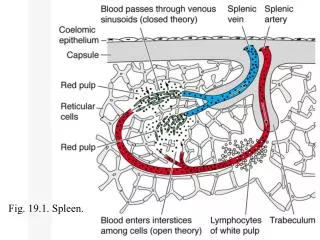
Consistency of the spleen -white and red pulp( cords & sinuses),marginal zone -trabeculae art., central art., pencillar artery -skimming effect -defense spleen & storage spleen
Function of the spleen 1-immune function .specific like igM production . Nonspecific( opsionstuftin,properdin) to phagocyte the bacteria, fungi. 2-filter function . macrophages catch bacteria specially pnumoccocci, H. influnzie, noncellular materials . 3-removal of effecte platelets, RBC bu Culling 4-Pitting, removing particular inclusions from RBCs like parasite of malaria, nucleated RBCs
Function cont. 5-iron reutilization 6-pooling 30-40% platelet. In splenomegaly may reach 80% 7-reservoir function in dogs 8-haematopoiesis up to 5monthes of intrauterine life
Investigations Depend on the type of the disease which causing splenomegaly, like : -blood disease …blood investigation -liver cirrhosis causing portal hypertention …LFT,OGD for esophageal variesis -associated with lymphadenopathy do LN biopsy
Investigation cont. 1-plain abdomen -calcification(s)( hydatid cyst, haemangioma, spleenicanurysm, TB, old infarct of SCA…etc.) -soft tissue shadow at upper lt. hypochonderial area -descending colonic gas shadows -obliteration of the psoas shadow
2-ultrasound -size and consistency -cystic or solid ? -rapture.. -haematoma -therapeutic i.e abscess drainage or aspiration of the cyst, biopsy!!!!
3-CT abdomen with or without contrast 4- MRI 5-radio-isotop scans Te 99 -recurrent disease? -position & site -RBC life duration and place of their destruction 6- angiography -embolization of selected cases of splenichge. -liver schirosis -before splenectomy to decrease its size
Congenital anomaly 1- absence -rare and it is usually associated with congenital heart disease and fatal sepsis. 2- accessory spleen ( splenuculi) -20% of population & 30% of pts. with haemolytic disease -no more than 2cm -80% found in splenichilum and vascular pedicle -omentum,gastrosplenicligament,splenocolicligament,stomach greater curvature, small & large bowel mesetery,in left broad ligament and spermatic cord…etc. -if not removed after splenectomy ,it cause recurrent of the disease
3-Hamartoma-1cm …huge size causing abdominal swelling-2 types arise from red and white pulp-incidentaly sometimes found by CT- abdomen 4- cysts -rare a-true one, non-parasitic -may be dermoid, mesenchymal inclusion cysts, epithelial cysts.
Cyst cont. B- false cysts .parasytic –echinococcus .seroma Clinical features: -asymptomatic -symptomatic .mass in lt. upper hypochonderial area Diagnosis: sonography of the abdomen Treatment: .depend on symptomes. if asyptomatic……observation and follow up by sonography. if symptomatic … depend on its size small one do excision large one unroofed if or do aspiration, drainage, sclerosing
Rapture of spleen Etiology; -direct trauma -without trauma in diseased spleen duo to malaria, infectiouse mononucleosis -iatrogenic during operation It is suspected when there is # ribs at lthypochonderial area.
Clinical features: 3 groups: 1- patient sccumbs rapidly from massive he. 2-initial shock ,recovery and later sings of internal bleeding. Kehrs sings, shifting dullness in flanks, rectal examination fullness in pelvis 3- delayed case
Investigations -plain abdomen -sonography of abdomen -CT-abdomen Treatment: Surgical options -splenectomy( total or partial) - splenorraphy -mesh net pressure compression
Infection of the spleen:- -rare -cause spontaneous rapture of spleen -duo to: - infectious mononucleosis, CMV -malaria -fungal infection -amylodosis, pregnancy, lymphoma, Q-fever…
Splenic infarction:- -duo to myloproliferative syndrome -vascular occlusion in sickle cell anemia, infected heart valves bacterial endocarditis -may be asymptomatic or causing abdominal pain in left hypochondrium, gaurdening, friction rub
Absces of the spleen:- -uncommon ,most common in tropical area -occurs with thrombosis of vessels or infarct of SCA. • Splenic thrombosis infected • Metastatic abscess duo to typhoid, paratyphoid, oestiomylitis, otitis media, pureperal sepsis -mechanism:- .haematological .contagious .haemoglobinopathy .trauma .immunosuppression
Symptomes:- -delayed -fever, pain left hypochondria, increase WBC, splenomegaly in 1/3 of the patients Diagnosis:- u/s or CT of abdomen Treatment:- drainage
Aneurysm of splenic artery:- -rare,< 1% -female : male is 2:1 -involve main trunk • May be single or multiple -asymptomatic unless ruptured -occasionally palpable in epigastrium with bruit in left hypochonderial area -incidentally on plain abdomen with calcified ring -usually < 45 years, ¼ pregnant at 3rd trimester. -in young females asymptomatic -maternal mortality high( 70 %) -treatment usually surgery by splenectomy