Download
1 / 26
260 likes | 603 Vues
TRAITEMENT DE LA COAGULATION INTRAVASCULAIRE DISSEMINE. Cécilia Tomescu II ème année DESC Saint Etienne juin 2009. Pourquoi traiter la CIVD?. Fourrier. CIVD+ 44. CIVD- 16. 22. 15. SAPSII. P<0,001. 77%. 32%. Mortalité. 4,2. Lactates. 6,4. Fourrier et al Chest 1992;101:816-23.

E N D
TRAITEMENT DE LA COAGULATION INTRAVASCULAIRE DISSEMINE Cécilia Tomescu IIème année DESC Saint Etienne juin 2009
Pourquoi traiter la CIVD? • Fourrier CIVD+ 44 CIVD- 16 22 15 SAPSII P<0,001 77% 32% Mortalité 4,2 Lactates 6,4 Fourrier et al Chest 1992;101:816-23 SAPSII
Pourquoi traiter la CIVD? • CIV obstrue la circulation • Consommation des facteurs de l’hémostase = hémorragies potentiellement mortelles • Les médiateurs de la coagulation aggravent les conséquences de l’inflammation
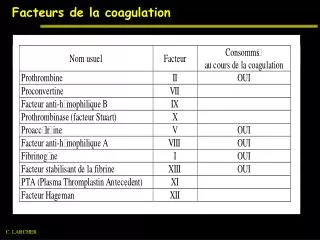
Situations cliniques à risque de CIVD • Induction de la synthèse et de l’expression membranaire de FT en réponse à des stimuli inflammatoires:sepsis, hypothermies, hyperthermies malignes, choc hémorragique • Contact entre FT constitutif extra-vasculaire et le FVIIa liée a une effraction vasculaire:traumatismes, complications obstétricales, brûlures, pancréatites, complications transfusionnelles, hémolyses • Contact entre FT et le FVIIa exprimé a la surface de cellules anormales:cancers métastasés, hémopathies malignes
Principes de traitment • Étiologique: primordial • Substitutif • Spécifique
Traitement substitutif • Transfusion plaquettaire (d) • <50 000 plaquettes/mm et facteurs de risque hémorragique: acte invasif, thrombopathie associée • Hémorragie grave • Plasma frais congelé (d) • TP< 35-40% et hémorragie/ acte invasif • Fibrinogène: pas d’indication (d) • Complexe prothrombique: contre-indiqué (d) XXIIème Conférence de Consensus: SFAR, SFH, GEHT, SFRUP CIVD en réanimation: définition, classification, traitement 2002
Traitement spécifique • Inhibiteurs de la voie du facteur tissulaire et concentrés de protéine C n’est pas validée (c) • Pas d’information sur l’efficacité du recombinant activé de la PC ( drotrecogine ) (d) • Antithrombine améliore la CIVD du sepsis (a) • Héparine: pas démontrée (c) • Modulateurs de la fibrinolyse: pas démontrée (c) XXIIème Conférence de Consensus: SFAR, SFH, GEHT, SFRUP CIVD en réanimation: définition, classification, traitement 2002
Antithrombine 2339 patients • KyberSept Randomisé, double aveugle, contrôlé, multicentrique 1157 placebo 1157 ATIII: bolus 6000UI, 30000UI/ 4j Mortalité J28 38,7% Mortalité J28 38,9% Mortalité J90 48,5% Mortalité J90 46,4%
Antithrombine P=0,04
Antithrombine • Kienast: étude rétrospective sur le résultats de l’étude KyberSept • Calcul du score ISTH pour CIVD; deux groupes: avec et sans CIVD • A inclus les patients n’ayant pas eu de héparine • 277 placebo, 286 ATIII Journal of Thrombosis and Haemostasis.2006. 4 (1): 90-7
Antithrombine • Kienast: résultats • Bénéfice en terme de mortalité à 90 jours pour le patients avec CIVD qui ont reçu ATIII • Pas de bénéfice pour le groupe sans CIVD • Augmentation de risque hémorragique ds le groupe sans CIVD (9,8%, rate 3,1%, p<0,05) • Non significatif pour le groupe avec CIVD Journal of Thrombosis and Haemostasis.2006. 4 (1): 90-7
Antithrombine 33 patients, bolus 6000 UI AT, puis 250 UI/h/4j
Antithrombine Pas de bénéfice en terme de mortalité Augmentation du risque de saignement
Protéine C activée • Prowess 1690 patients 850 Drotrecogin 840 placebo Mortalité J28 24,7 Mortalité J28 30,8 • Risque relatif 19,4%, 95%CI, 6,6-30,5 • Risque ratio 6,1%, p=0,005 Saignement majeur 3,5% Saignement majeur 2%
Protéine C activée • JF Dhainaut: analyse rétrospective des données Prowess pour les patients avec CIVD N Placebo Drotrecogine 30,8% 24,7% 1690 Overall 30,5% 43,0% 454 Overt DIC No overt DIC 22,1% 27,1% 1114 0,5 0,6 0,7 0,8 0,9 1,25 1,67 2 Relative Risk of Death ( Point Estimate and 95% CI
Protéine C activée • JF Dhainaut Serious bleeding 28-days NS
Protéine C activée 48% non respect contre-indications => saignement
Héparine Levi XPress
Héparine • Haley Prowess KyberSept Optimist Placebo Avec héparine Sans héparine Haley M. Current Opinion in Infectious Diseases 2004; 17:205-211
Héparine Haley Harmfull No effect Benefit Prowess KyberSept Optimist Overall 0,37 0,61 1,65 2,72 Heparine beneficial in all placebo groups P<0,0001
Conclusion • CIVD associé au mauvais pronostic Voies de recherche Ttt étiologique SFAR Surveinving sepsis Ttt substitutif