Download
1 / 53
530 likes | 726 Vues
HCV update. Ardis Ann Moe UCLA CARE clinic/NEVHC Van Nuys 21 June 2014 amoe@mednet.ucla.edu. Goals:. 1) terminology of hep C 2) benefits of hep C treatment 3 )drug interaction issues with HIV meds

E N D
HCV update Ardis Ann Moe UCLA CARE clinic/NEVHC Van Nuys 21 June 2014 amoe@mednet.ucla.edu
Goals: • 1) terminology of hep C • 2) benefits of hep C treatment • 3)drug interaction issues with HIV meds • My thanks to my colleague Debika Bhattacharya for use of her slides for this presentation.
Hep C viral load is not the same as HIV viral load • Hep C viral load does not correlate with risk of death, cirrhosis, liver damage.
Hep C can be cured with current medications, unlike HIV. • Cure=SVR “sustained virological response” • Hep C viral load 6 months after completing treatment is undetectable = SVR
CHILD score: A, B or C.(also scored numerically:5 or more points) • Risk of death from cirrhosis. • Only to be used in patients with documented cirrhosis • Important since simeprevir contraindicated in patients with CHILD score>5.(or B or C) • Website for calculator for CHILD score: • :http://www.mdcalc.com/child-pugh-score-for-cirrhosis-mortality/
Patients who do develop cirrhosis have many problems: • Esophageal varices and recurrent internal bleeding • Ascites (fluid on the abdomen) • Brain damage from hepatic encephalopathy • liver cancer • Problems with medications • Leg edema • Jaundice
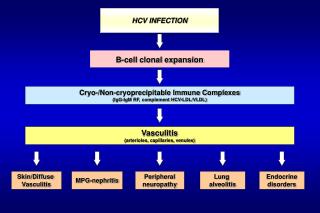
Even without cirrhosis, there are complications of hep C • Fatigue • Cryoglobulimia (kidney damage) • Porphyria cutaneatarda • Increased risk of diabetes
Treatment of hep C reduces or eliminates risk of liver cancer, cirrhosis, cryoglobulinia, and porphyria. • However, cirrhosis is permanent scarring, so once there is cirrhosis, there is always some risk of liver cancer in the future, even if hep C cured. • Treatment of hepatitis C also appears to alleviate fatigue. Hepatology.2014 Apr 5
HCV DAA (direct acting antiviral) Cheat Sheet • PREVIR • Protease inhibitors: telaprevir, boceprevir, simeprevir • BUVIR • Polymerase inhibitors • Sofosbuvir • ASvir • NS5A inhibitors: Daclatasvir, ledipasvir
IDSA Recommendations • IFN-free: • Genotype 1: Sim/Sof x 12 weeks (+/- ribavirin) • Genotype 2: Sof/ribavirin x 12 weeks • Genotype 3: Sof/ribavirin x 24 weeks • Genotype 4: Sof/rifabirin x 24 weeks
Side effects: • Simeprevir • Rash including photosensitivity (28%), itching (22%), nausea (22%), shortness of breath (12%), elevated bilirubin (49%) • Note rash more likely in patients with cirrhosis
Side effects • Sofusbuvir • Fatigue 59% • headache 36% • insomnia 25% • chills 17% • irritability 13% • rash 18% • itching 27% • nausea 34% • diarrhea 11%
Overall <5% of study subjects stopped sofosbuvir and simeprevir on the COSMOS and other studies because of side effects.
Hep C meds to be approved • Daclatasvir: effective against genotypes 1,2,3 Ledipasvir: effective against genotype 1; to be combined with sofosbuvir into 1 pill a day
find those patients who need to be treated NOW with simeprevir/sofosbuvir, and who are willing to be on a limited HIV regimen (complera, isentress, truvada) in order to prevent drug interactions • Patients who are on Atripla, Stribild, or boosted protease inhibitors will have to wait until more hep C drugs available.
Treat HIV first if CD4 <500 and get HIV viral load <50 copies for maximal response from hep C meds • If CD4 count >500, may be able to wait on starting HIV meds until after hep C treatment completed.
Obtain baseline hep C viral load (within 3 months of beginning treatment) • Counsel patient on need to take all meds • Counsel patient on need to avoid sunlight, risks of nausea and rash • Alter patient’s HIV regimen if necessary.
Follow-up 2 weeks and at 4 week point after initiating hep C meds to check on adherence and immediate side effects. Mild rash can be treated through with benedryl, topical steroids • Check CBC, platelets, AST, ALT every 2 weeks during first 4 weeks. • Repeat Hep C viral load at Week 4 point
Hep C viral load should be <25 copies at Week 4 point; if not, patient may need to be discontinued to prevent resistance. • Recheck hep c viral load at Week 8. • If hep c meds tolerated, see patient at Week 4, Week 8 and Week 12 and check CBC, platelets, AST, and ALT at each visit(or monthly if being treated x 24 weeks)
If patient on ribavirin containing regimen, dose reduce ribavirin if anemia develops: Hb < 10 • Most anemia with Sof/ribavirin mild.
Repeat Hep C viral load 6 months after completing therapy to ascertain cure: “SVR”.
Audience Response Question: Which is FALSE 1)hep C viral load of 2,000 copies may be a patient undergoing self-cure 2)a patient who is cured of hep C but still has cirrhosis has no risk of liver cancer 3)simeprevir has multiple drug interactions with many HIV medications 4)patients cured of hep C have less fatigue
Study of reinfection rates • 191 MSM with cured (treated with meds) or spontaneously cleared hep C • 44 were reinfected • 8 were infected several more times • Same or different genotypes • None had IDU risk factor • Estimated that 25% will be re-infected within 2 years of cure. • AIDS 2013 Oct 23;27(16):2551-7
Prison populations in Spain: • 119 Hep C Ab+, cured or spontaneously cleared while as inmate. 81% hx of IDU • Reinfection rate 5.37 per 100 person years, higher in active IDU and HIV co-infected • J Hepatology. 2013 July;59(1):45-51
Selection of patients for hep C treatment will have to include safe sex counseling and sobriety