Download
1 / 26
260 likes | 504 Vues
Dhr. S. M C R Geb. 19-10-88. Patiëntendemonstratie 13-07-05 Dorus Fennis azM Neurologie. Anamnese. Presentatie op SEH vw onwelwordingen. Op achterbank auto enkele aanvallen met schokken en bewustzijnsverlies 30 minuten. Lft. 17 jr. Enkele dagen hiervoor een stuk hout op hoofd. Anamnese 2.

E N D
Dhr. S. M C RGeb. 19-10-88 Patiëntendemonstratie 13-07-05 Dorus Fennis azM Neurologie
Anamnese • Presentatie op SEH vw onwelwordingen. Op achterbank auto enkele aanvallen met schokken en bewustzijnsverlies 30 minuten. • Lft. 17 jr. • Enkele dagen hiervoor een stuk hout op hoofd.
Anamnese 2 • VG: blanco. • Med; geen. • Intox: enkele malen per week cannabis. Overigens ??? • Soc: woont bij moeder. • Fam.A.: epilepsie-.
Neurologisch onderzoek • P. 144/min., RR=148/68 mmHg, T=38.1 • Hyperventilerend, geagiteerde indruk. • E4M6V5. Kleine schaafwond links frontaal. • VZR rechts neigend tot Babinski, links plantair.
Anvullend onderzoek • Lab: Leuco’s 15.9. • Astrup: 7.64-2.8-27-22-3.1-10.5-98% • ECG; sinustachycardie. • EEG; geen epileptiforme activiteit
Diagnose en beleid • Werkdiagnose: pneumencephalie met gegeneraliseerde convulsieve status epilepticus (passagère). • Beleid: opname en AED. • Plan: MRI en EEG.
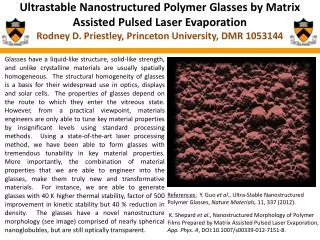
Conclusie • Gebarsten dermoïd -cyste. • Epilepsie t.g.v. dermoïd? Intoxicaties?
Beloop • Tijdens opname geen insulten meer. Wel veel hoofdpijn en braken. Geleidelijk herstel. • Tijdens follow-up zeer matige therapie-trouw. Enkele malen opname vw. insulten waarbij subtherapeutische spiegels AED. • Overleg neurochirurg: expectatief. • Intoxicaties met benzodiazepinen, cannabis en cocaïne. • Controle MRI’s conform eerste MRI. • Lost to follow-up.
Dermoid cysteepidemiologie • 0,04-0,6% van intracraniele tumoren. • Geen verschil geslacht gevonden. • Piekleeftijd van ontdekken onduidelijk • 2e-3e decade? • 30-50 jaar?
Dermoïd cystePathofysiologie • Inclusie van ectoderm tijdens sluiten neurale buis (4e –5e wk). • Typisch midline (sella). • Inhoud: talg en zweet klieren, haar follikels, soms tanden en nagels. Geen vet! • ‘Vet’ op MRI is keratineus debris en cholesterol.
Embryologie • Mesodermal elements must be incorporated into developmental and similar lesions for adipose tissue to be present. This is the case for some teratomas but not dermoid/epidermoid inclusion cysts. • Germ layer Mature tissue • Ectoderm Skin, teeth, nails, neuroectoderm • Mesoderm Adipose, bone, cartilage, muscle • Endoderm Lining epithelium, exocrine glands, solid organs
Dermoïd cysteKlinische verschijnselen • Afhankelijk van plaats, expansie en al of niet ruptureren. • Typisch: hoofdpijn, epileptische aanvallen. • Bij barsten (spontaan of traumatisch) chemische meningitis of ventriculitis. • Soms ook ischemie tgv vasospasmen. • Zelden obstructieve hydrocephalus. • In ASG; relatie met dysraphisme?
Dermoid cystediagnostiek • CT: hypodense laesie, scherp begrensd. Soms calcificaties. • MRI: T1 hyperintens, T2 hypointens • ‘Vetdruppels’ in arachnoidale ruimte en/of ventrikels • Meningeale aankleuring
Dermoid cysteDD. • Epidermoid cyste • Vaker voorkomend • Soms op hogere leeftijd, secundair aan ‘implantatie’ • Op dermale fusieplaatsen • Minder progressieve groei, exfoliatief en niet expansief. • Geen klierelementen. • MRI: T1 hypointens.
Dermoid cysteBeleid • Chirurgie: resectie. • Cave: vastgoei aan omgevende structuren • Symptomatisch
Dermoid cystePrognose • Prognose wordt als goed omschreven. • Cijfers zijn niet voorhanden. • Lijkt niet afhankelijk van grootte. • Lijkt niet afhankelijk van ruptuur. • Na chirurgie geen neiging tot recidiveren, ondanks subtotale resectie.
Literatuur • Johnson DG e.a. Ruptured ‘giant’ supratentorial dermoid syst. J Clin Neurosc (2005);12:198-201 • Oursin C e.a. Ruptured intracranial dermoid cyst. J Neurosurg Sc (1999);43:217-221 • Bradley • Neuroimaging. Clinical and Physical Principles. Zimmerman, Gibby & Carmody. Springer 2000.