Download
1 / 37
650 likes | 1.98k Vues
Cataract and Uveitis. Mohammad Ghoreishi , MD. Cataract and Uveitis. Uveitis , as complication of cataract Cataract, as complication of uveitis Cataract surgery and uveitis. Uveitis as complication of cataract. Phacoanaphylactic endophthalmitis Phacotoxic uveitis

E N D
Cataract and Uveitis Mohammad Ghoreishi, MD
Cataract and Uveitis • Uveitis , as complication of cataract • Cataract, as complication of uveitis • Cataract surgery and uveitis
Uveitis as complication of cataract • Phacoanaphylacticendophthalmitis • Phacotoxicuveitis • Phacolythic glaucoma and uveitis
Phacoanaphylacticendophthalmitis • Immunologic type response to lens protein release after injury to the lens capsule or after cataract surgery • Rarely spontaneous lens capsule rapture may cause the disease
Pathogenesis • Autologous lens protein may become autoantigenic after exposure to the aqueous humor • Usually abrupt onset, but may be insidious • Early onset in previously sensitized patients
Pathology • Zonal granulomatous inflammation centered at the site of lens injury
Clinical findings • Mutton-fat KPs • Congested iris vessels • Posterior synechiae • Dense flare and cells
Treatment • Corticosteroids • Cycloplegic • Surgical removal of lens material
Phacotoxicuveitis? • Supposed toxic effect of lens material • May be a less severe form of phacoanaphlaxis
Phacolytic glaucoma (PG) • Phacolytic glaucoma (PG) is the sudden onset of open-angle glaucoma caused by a leaking mature or hypermature (rarely immature) cataract • It is cured by cataract extraction
Phacolytic glaucoma • Occurs in cataractous lenses with intact lens capsules • Direct obstruction of outflow pathways by high molecular weight lens proteins released from microscopic defects in the lens capsule • Macrophagic response to lens protein in the anterior chamber, but not the cause of the outflow obstruction
History • History of slow vision loss for months or years prior to the acute onset of pain, redness, and sudden decrease in vision (vital clue to the correct diagnosis) • Symptoms mimic acute angle-closure glaucoma
Clinical findings • Severly elevated IOP • Microcystic corneal edema, and the anterior chamber contains • Intense AC reaction, flare and large cells (macrophages) • Aggregates of white material, and iridescent or hyperrefringent particles in AC (calcium oxalate and cholesterol crystals liberated from the degenerating cataractous lens) • No keratic precipitates (unlike phacoanaphylacticuveitis
Clinical findings • The anterior capsule of the lens frequently is dotted with patches of soft white material • In contrast to some forms of lens-induced glaucomas (eg, lens particle glaucoma, phacoanaphylactic glaucoma), the lens capsule is grossly intact • Gonioscopy findings usually are normal; however, evidence of old angle recession was found in 25% of eyes in one study
Causes • Mature cataract (totally opacified) • Hypermature cataract (liquid cortex and free-floating nucleus) • Focal liquefaction of immature cataract (rare) • Dislocated cataractous lens in vitreous
Differential diagnosis • Intumescent Lens Glaucoma • Acute Angle Closure Glaucoma • Lens-Particle Glaucoma • Uveitic Glaucoma (Pahcoanaphylactic) • Neovascular Glaucoma • Phacomorphic Glaucoma • Dislocated cataractous lens in vitreous
Treatment Aggressive antiglaucoma therapy Corticosteroid Cataract surgery as soon as IOP is controlled and inflammation subsided
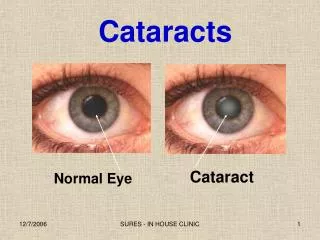
Cataract caused by uveitis • Cataract formation is a common complication of chronic or recurrent uveitis. • It is caused by the inflammation itself, or by the steroid and glaucoma • The incidence of cataract approaches 50%. • The most common type of cataract in uveitis patients is the posterior subcapsular opacity
Physiopathology • Thought to be the result of prolonged breakdown of the blood-ocular barriers caused by intraocular inflammation. • The entry of plasma phospholipids, or its precursor, into the eye is thought to increase lens epithelial permeability
Cataract surgery in uveitis • Preopperative measures • Intraoperative • postoperative
Cataract surgery in uveitis • The clinical course, management, complications and visual outcome of uveitic cataract are directly related to the type and cause of uveitis • Preoperative diagnosis of the etiology and proper management of uveitis and its etiology, are essential prognostic factors for treating cataract
Cataract surgery in uveitis Patient selection for surgery • Visually significant cataract • Fully controlled inflammation • Predicted substantial improvement in visual acuity
First, infectious and treatable causes of uveitis must be identified. • Treatable causes, such as syphilis, TB, Toxo, viral, parasitic …, should be managed before surgery
Second, many forms of uveitis are associated with systemic diseases such as HLA-B27-associated diseases, Behcet disease, sarcoidosis, systemic lupus erythematosis, rheumatoid arthritis... • Systemic causes of uveitis must be identified and treated, or controlled preoperatively
Third, the surgical outcome may be influenced by the type of uveitis. • Fuchs heterochromiccyclitis has historically been thought to have a good prognosis after cataract surgery even with incomplete control of anterior chamber cell • Conversely, cataract surgery in patients with JIA related uveitis and Behcet disease carries poor visual outcome
Controlling inflammation • Clinically significant inflammation has been defined as 1+ cells (5 to 10 cells) according to the criteria of Hogan • Total control of active inflammation (0 to 2 in anterior chamber or vitreous body) for at least 3 months • Aqueous flare in the chronic uveitic patients simply denotes vascular incompetence of the iris and ciliary body, a consequence of vascular damage from the chronic or recurrent uveitis. • Therefore, flare should in general not be used as a guide for control of inflammation
Controlling inflammation • Specific treatment • Treating the infectious etiology: antivirals, antibacterials, antiparasitics.. • Treating noninfectious etiology • Nonspecific • Corticosterroids • Cytotoxics and immunosupressants • NSAIDS
Concomitant pathologies Concomitant ocular pathologies should be diagnosed and addressed, including • Retinal detachment • Optic atrophy • Vitreous opacity • Cystoid Macular edema • Epiretinal membranes • Corneal problems such as scarring,band shape keratopathy, stromal thinning, Intra-stromal hyaline- or lipid-like deposits.
Intraoperative • Proper Surgical technique • Treating iris and pupil abnormalities such as miosis, synechiae, PAS • Managing anterior and posterior capsule • Eradicating all cortical and nuclear material • Avoiding too much manipulation • Avoiding irritant substances • Combined corneal or vitreoretinal surgery • Periocular or intraocular injection
IOL • Indications, when to avoid IOL implantation • There is general agreement about avoiding an IOL in, a patient with JRA-associated uveitis. • Behcet disease ? • Recurrent, poorly controlled uveitis
Iol • Position • Minimize haptic-uveal contact • Avoid AC IOL • Avoid sulcus implantation • A PCIOL implant resting on the ciliary body or an • IOL design and material • Single piece • Hydrophobic vshydrophylic • Capsular and uveal compatibility • Avoid silicone material • Heparine coated IOL
Postoperative • Uveitis as complication of cataract surgery • Other complications related to cataract surgery and uveitis
Complications after cataract surgery • Recurrence of inflammation • CME • PCO and capsular contracture • IOL deposit • Hypotony
Uveitis secondary to cataract surgery • Severe postoperative inflammation is more common after cataract surgery in eyes with uveitis • Early onset • TAAS • Lens induced • Late onset • Infectious: Propiony Bacterium Acne • UGH
Early postoerative inflammation • Diagnosis and eradicating or treating the causes • In addition to intensive topical, periocular, or even systemic • anti-inflammatory treatment, the injection of recombinant tissue plasminogen activator (10 μg in 0.1 mL buffered saline solution) into the anterior chamber may help disperse • Be caution about early surgical or Yag-Laser manipulation in case of fibrin formation
Conclusions • Cataract and glaucoma are frequently associated with each other as cause and effect • Cataract surgery in a patient with uveitis requires thorough diagnostic investigation, diligent perioperative control of inflammation, and meticulous surgical technique • Proper surgical technique, choice of IOL and postoperative control of inflammation and complications can lead to satisfactory visual outcomes after cataract surgery in uveitis patients, and prevention of uveitis in normal subjects