Download
1 / 91
910 likes | 1.68k Vues
HIPERPLASIA ENDOMETRIAL. Dra. Silvia Fabiola Estrada Rivera R1 Ginecología Oncológica COORDINADOR: Dr. David Francisco Cantú De León. TÓPICOS. HISTORIA. HISTORIA. Marsden DE, Hacker NF. The Classification , Diagnosis And Management Of Endometrial Hyperplasia . 2003;3:89-97. HISTORIA.

E N D
HIPERPLASIA ENDOMETRIAL Dra. Silvia Fabiola Estrada Rivera R1 Ginecología Oncológica COORDINADOR: Dr. David Francisco Cantú De León
HISTORIA Marsden DE, Hacker NF. TheClassification, Diagnosis And Management Of Endometrial Hyperplasia. 2003;3:89-97.
HISTORIA Marsden DE, Hacker NF. TheClassification, Diagnosis And Management Of Endometrial Hyperplasia. 2003;3:89-97.
EMBRIOLOGÍA 6 SDG ESTROGENOS Maternos Placentario 8-9 SDG Lagman. Embriología Médica Con Orientación Clínica. Ed. Panamericana. 10ª Edición.
EMBRIOLOGÍA Invaginación Lagman. Embriología Médica Con Orientación Clínica. Ed. Panamericana. 10ª Edición. Bergeron C. Histología Y Fisiología Del Endometrio Ginecología-obstetricia Elviser 2006
ANATOMÍA Peso: 90 gr Fondo Tamaño: Largo: 7.5 cm Ancho: 5 cm Grosor: 2cm cuerpo CÉRVIX Moore KL. Anatomía Con Orientación Clínica. Ed. Li Ppicontt Williams & Wilkins.6 Ta Edición. 2010
Situado: Vejiga – Recto ANATOMÍA Posterior: Repliegue rectouterino Colon signoides y recto Anterior: Fondo de saco vesicoterino Vejiga Lateral: Ligamento ancho Ligamentos cardinales Ureter Arteria uterina Moore KL. Anatomía Con Orientación Clínica. Ed. Li Ppicontt Williams & Wilkins.6 Ta Edición. 2010
ANATOMÍA Irrigación Drenaje venoso Plexo venoso A. Uterina Superior: Vena uterina Inferior Pudenda interna Plexo hemorroidal o rectal Plexo vesical Venas ováricas y venas de ligamento redondo • Arteria Uterina • Arteria ovárica Moore KL. Anatomía Con Orientación Clínica. Ed. Li Ppicontt Williams & Wilkins.6 Ta Edición. 2010
ANATOMÍA Arterias Arcuatas Arterias Basales Arterias Espirales C. Bergeron. Histología Y Fisiología Del Endometrio Normal. Ginecología-obstetricia. Elviser. 2006
ANATOMÍA Plexo Hipogástrico Inferior: Ramas T 10-12 L1 Nervios Esplácnicos Ramas S2-4 Fibras parasimpáticas Plexo Útero-vaginal: Ligamento Ancho Fibras Simpáticas SkandalakisSurgicalAnatomy. 2004 Anatomía Con Orientación Clínica Moore 2003.4ta Edición
FISIOLOGÍA C. Bergeron. Histología Y Fisiología Del Endometrio Normal. Ginecología-obstetricia. Elviser. 2006
HISTOLOGÍA C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006
HISTOLOGÍA C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006
HISTOLOGÍA C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006
HISTOLOGÍA C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006
BIOLOGÍA MOLECULAR Receptores de Estrógenos ↑↑ Periodo preovulatorio y ovulatorio precoz • ERa • Proteína de 595 aa • Erβ • Proteína de 485 aa • La síntesis depende de los estrógenos • Núcleos glandulares • Células del estroma • Células musculares lisas de los vasos endometriales C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006 Seminars in Diagnostic Pathology, Vol 27, No 4, November 2010
BIOLOGÍA MOLECULAR Receptores de Progesterona Punto Máximo: Mitad del ciclo menstrual Ausentes: Fase lútea (excepto en el estroma) • PRA • 94 kDa • PRB • 114 kDa • 50% en cáncer de endometrio C. Bergeron. Histología y fisiología del endometrio normal. Ginecología-Obstetricia. ELVISER. 2006 Seminars in Diagnostic Pathology, Vol 27, No 4, November 2010
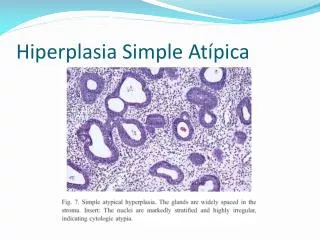
DEFINICIÓN • Conjunto heterogéneo de lesiones patológicas que van desde proliferaciones reversibles hasta lesiones precursoras de cáncer. • Proliferación glandular con forma y tamaño irregular con un aumento en la relación glándula/estroma del endometrio. Ben E. Montgomery. Endometrial Hyperplasia: A Review. Obstetrical and GynecologicalSurvey. 2004:59 Mills AM, Longacre TA. Endometrial Hyperplaisa..Seminars in DiagnosticPathology. 2010;27: 199-214
EPIDEMIOLOGÍA Mujeres entre 18-90 a con patología endometrial Miembros del grupo de salud Estado de Washington Incidencia global 133 por c/ 100,000 mujeres por año Reed SD, Newton, KM; Clinton WL, et al. Incidence of endometrial hyperplasia. Am J ObstetGynecol 2009;200:678.e1-678.e6
Epidemiología Armstrong AJ. Diagnosis and Management of Endometrial Hyperplasia. Journal f MinimallyInvasiveGynecology. 2012;19.
PATOGENIA Hiperplasia Endometrial Cáncer de endometrio Molecular Profiling Of Endometrial Malignancies .Obstetrics And Gynecology International Volume 2010
PTEN Espindola D, Kennedy KA, Fischer EG. Management of AbnormalUterineBleeding and thePathology of Endometrial Hyperplasia. ObstetGynecolClin N Am. 2007;34:717-737
Molecular Profiling Of Endometrial Malignancies .Obstetrics And Gynecology International Volume 2010
MIS (INESTABILIDAD DE MICROSATÉLITES) • Perdida de la reparación de los genes • Evento temprano en la carcinogénesis Corrección de errores de replicación del DNA MIS Formación tumoral Espindola D, Kennedy KA, Fischer EG. Management of AbnormalUterineBleeding and thePathology of Endometrial Hyperplasia. ObstetGynecolClin N Am. 2007;34:717-737
PREVALENCIA DE ALTERACIONES MOLECULARES MUTACIÓN PTEN MUTACIÓN K-ras INEST. MICROSATÉLITES MUTACIÓN B-CATENINA Moore E, Shafi M. Endometrial Hyperplasia. Obstetrics, Gynaecology And Reproductive Medicine. 2013 23:3
Patogenia MLH1 METILACIÓN Pten Msi kras hiperestrogenismo Pten Msi Kras B-catenina pik3ca P53 HER 2 P53 P16 HER2 Msi E-caderina pik3ca Molecular Profiling Of Endometrial Malignancies .Obstetrics And Gynecology International Volume 2010
PATOGENIA Moore E, Shafi M. Endometrial Hyperplasia. Obstetrics, Gynaecology And Reproductive Medicine. 2013 23:3
FACTORES DE RIESGO Weber am, belinsonjl. Riskfactorsfor endometrial hyperplasia and canceramongwomenwhithabnormal. Bleeding. Obstetrics and gynecology. 1999 Chen YL, Wang KL, Chen MY. Risk factor analysis of coexisting endometrial carcinoma in patientswith endometrial hyperplasia:aretrospective observacional study of taiwaneseGynecologicOncologyGroup. 2013;24
OBESIDAD GokhanAcmaz Et Al. Evaluation Of Endometrial Precancerous Lesions In Postmenopausal Obese Risky Women Asian Pacific Journal Of Cancer Prevention, Vol 15, 2014 Armstrong AJ. Diagnosis And Management Of Endometrial Hyperplasia. Journal F MinimallyInvasiveGynecology. 2012;19.
Niveles elevados de insulina: EH, EC IMC 25.5: EH TG: EC Edad: 44 a IMC: 24 CONCLUSIÓN: Hiperinsulinemia esta asociada a EH C/S atipias Probablemente sea una pieza importante que promueva los lesiones hiperplásicas. GynecologicOncology 2014;132: 606-6010
G. Vorgias 240 Et Al. / European Journal Of Obstetrics & Gynecology And Reproductive Biology 125 (2006) 239–242
45 Estudios 38,702 mujeres en txminimo por 12 meses • Tipos de estudios • Estrógenos sólos • Estrógenos/Progestágenos combinados vs placebo • Estrógenos sólos vs Estrógenos/Progestágenos combinados (secuenciales ó combinados) • Estrógenos/Porgestágenos continuos vs Estrógenos/Progestágenos secuenciales Hormone Therapy in postmenopausalwomen and risk of endometrial hyperplasia( Review) 2010 The Cochrane Collaboration.
20 -50% Riesgo de HE en TRH sin oposición Se asocio con un aumento significativo del riesgo de HE a los 2 a 3 años La TRH en mujeres postmenopáusicas se debe realizar con estrógenos y progesterona. Hormone Therapy in postmenopausalwomen and risk of endometrial hyperplasia( Review) 2010 The Cochrane Collaboration.
ANOVULACIÓN CRÓNICA Proliferación endometrial Woodburn R. Diagnosis and Management of Endometrial Hyperplasia. PostgraduateObstetrics & Gynecology. 2014
SOP • 25% SOP Hiperplasia endometrial • Prevalencia de obesidad: 63.7% Obesas 30% intolerancia a la glucosa 10 % DM2 Delgadas 10% intolerancia a la glucosa 1.5 % DM2 Human ReproductionUpdate, 2001 Vol. 7 522-255 PolycisticOvarySyndrome: UpdateOn Diagnosis And Treatment . The American Journal Of Medicine. 2014
SOP Obesidad DM2 Amplitud Pulsos LH Andrógenos Hiperinsulinemia Resistencia Insulina Ovario Androstenediona Testosterona Adrenal DHEAS GFHS IGFBPS-1 Transporte de Glucosa P450 Fosforilación del receptor de serina del receptor de insulina Testosterona libre Estradiol IGF 1 Best Practice & Research Clinical Endocrinology & Metabolism:. 2006
TAMOXIFENO • Modulador selectivo de los receptores de estrógeno • Aumento de riesgo en postmenopáusicas • Tiempo del tratamiento • Dosis • Hiperplasia endometrial, pólipos endometriales, carcinoma y sarcoma Cohen I. Endometrial Pathologies Associated With Postmenopausal Tamoxifen Treatment. Gynecologic Oncology 94 (2004) 256–266
TAMOXIFENO HIPERPLASIA ENDOMETRIAL EN PACIENTES POSTMENOPÁUSICAS CON CÁNCER DE MAMA EN TRATAMIENTO CON TAMOXIFENO Cohen I. Endometrial Pathologies Associated With Postmenopausal Tamoxifen Treatment. Gynecologic Oncology 94 (2004) 256–266
TAMOXIFENO HIPERPLASIA ENDOMETRIAL EN PACIENTES POSTMENOPÁUSICAS CON CÁNCER DE MAMA EN TRATAMIENTO CON TAMOXIFENO C/S SUA Cohen I. Endometrial Pathologies Associated With Postmenopausal Tamoxifen Treatment. Gynecologic Oncology 94 (2004) 256–266