Download
1 / 30
410 likes | 635 Vues
Purulent disease of the lungs and pleura. Diseases of the esophagus. L. Yu. Ivashchuk. ACUTE SUPPURATIVE DISEASES OF LUNGS Abscessing pneumonia - multiple destructive foci 0,3-0,5 cm in size, within 1-2 segments of lungs.

E N D
Purulent disease of the lungs and pleura. Diseases of the esophagus. L. Yu. Ivashchuk
ACUTE SUPPURATIVE DISEASES OF LUNGS Abscessing pneumonia - multiple destructive foci 0,3-0,5 cm in size, within 1-2 segments of lungs. Abscess of lungs - purulent or ichorous destruction of pulmonary tissue with formation of one or several cavities, filled by pus, and detached from adjacent parenchyma by a pyogenic capsule. Gangrene of lungs – a diffuse purulent, ichorous necrosis of the tissue without the tendency to demarcation with prompt spreading of necrotic zone and destruction of the parenchyma.
Etiology and pathogenesis • disturbances of bronchial patency with the development of atelectasis; • infectious inflammatory process in a pulmonary tissue; • regional disturbances of blood supply with a further necrosis of areas of pulmonary parenchyma.
Symptomatology and clinical course • Signs of a lobar pneumonia • Signs of intoxication (general weakness, headache, malaise, suppressed appetite, moderate chest pain, dyspnea, subfebrile temperature). • Troubling cough and dyspnea.
Objective signs • By percussion – a blunted sound over the site of the purulent focus and perifocal infiltration (at subpleural location of the abscess). • By auscultation – rough respiration with a moist rales in the zone of purulent focus. • After abscess discharge could be revealed bandbox sound by percussion, by auscultation - moist rales on the background of amphoric respiration.
Differential diagnosticof lung abscess with central lung carcinoma
Differential diagnosticof lung abscess with peripheral lung carcinoma
Complications: • pulmonary bleeding; • pyopneumothorax; • pleural empyema; • sepsis; • bronchogenic dissemination.
PULMONARY BLEEDING • I degree – hemorrhage less 300 ml. • ІІ degree – hemorrhage less 700 ml. • ІІІ degree - hemorrhage exceeds 700 ml. TREATMENT 1. Stop the cough 2. Decrease the pulmonary blood pressure 3. Hemostatic therapy
Tactics and choice of treatment • 1. The adequate antibacterial, antiinflammatory therapy • 2. Evacuation of purulent content of the cavities: • active sanation of tracheobronchial tree; • repeated punctures or external draining of peripheral cavities. • 3. Detoxycation therapy
4.Immune correction: • 5. Desensitizing, antiinflammatory therapy, regulation of activity of proteases (antihistamine, nonsteroid antiinflammatory agents, inhibitors of proteases, antioxidants). • 6. Correction of dysfunction of the vital organs and systems, prevention of complications, symptomatic therapy.
Indications for operative management in acute destructive processes of lungs: • Pulmonary bleeding of ІІ- ІІІ degree; • Progression of the process on the background of active and appropriate therapy; • Tension pyopneumothorax, which is failed to liquidate by the draining of a pleural space; • Impossibility to rule out the suspicion on a malignant tumour.
Contraindications • decompensation of the vital functions in the terminal stage, • bilateral purulent destruction of lungs, • concomitant incurable malignant tumours.
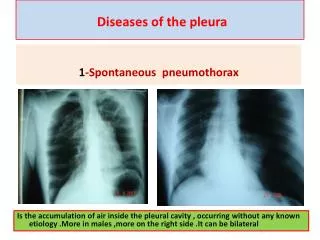
PLEURAL EMPYEMA The pleural empyema is a purulent inflammation of visceral and parietal pleural membranes, which is associated with accumulation of pus in a pleural space.
Etiology and pathogenesis • purulent and destructive processes of lungs, • abscesses of abdominal cavity (secondary pleural empyema), • open and closed damages of chest, • operative approaches on thoracic organs (primary pleural empyema). A secondary pleural empyema occurs in 88 % of the patients.
Classification • І. According to the pathogenic factor: • Primary. • Secondary. • ІІ. According to the clinical course: • Acute. • Chronic. • ІII. According to extension of the process: • Focal. • Wide-spread.
CLINICAL MANIFESTATION • Pain • Dyspnea • Cough • Intoxication • By palpation – diminished vocal fremitus on the side of lesion. • By percussion over the exudate it is possible to reveal short sound. • By auscultation – diminished or absent sound.
EMPYEMA FLUID CHARACTERISTICS pH < 7.0Glucose < 40 mg/dLLDH (lactatdehydrogenasa) > 1000 IU/dLPositive culture (50%)Specific gravity > 1.018WBC (leucocytes) > 500 cells/mm3Protein > 2.5 g/dL
Tactics and choice of treatment • The presence of pus in a pleural space is the indication for its elimination. In the place of performed diagnostic thoracentesis carried out the draining of empyema's cavity, its sanation by means of antiseptic solutions. In a focal empyema the aspiration of pus is performed by thoracentesis and only in its inefficiency carried out a draining of pleural space. • Intensive antibacterial and antiinflammatory therapy.
OPERATIVE APPROACH • INDICATION • transformation into the chronic form, that is in case of residual empyema's cavity. • VOLUME OF THE OPERATION • pleurectomy, decortication of lung. • In some cases, when a bronchial fistula and great empyema's cavity has been formed, there is the necessity of performance of resection of lung and corrective thoracoplasty.