Download
1 / 29
290 likes | 428 Vues
A Fresh Outlook on Osteoarthritis and Physical Capabilities. Randy Raugh, PT, DPT. Osteoarthritis (OA). 37.4% > age 60 with knee OA 2030 - 25% of Americans Leading cause of immobility/disability > 60 Symptoms: pain, stiffness, noisy and local swelling “Wear and tear?” CDC:

E N D
A Fresh Outlook on Osteoarthritis and Physical Capabilities Randy Raugh, PT, DPT
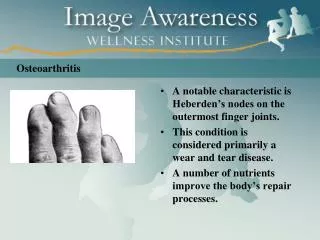
Osteoarthritis (OA) • 37.4% > age 60 with knee OA • 2030 - 25% of Americans • Leading cause of immobility/disability > 60 • Symptoms: pain, stiffness, noisy and local swelling • “Wear and tear?” • CDC: • “Incurable, progressive and degenerative”??? • “…focal and progressive loss of the hyaline cartilage of joints, underlying bony changes.” • A “disease” or a Mechanical problem? • A cartilage problem?
CDC • OA knee: 1 of 5 leading causes of disability among non-institutionalized adults. • ~ 80% of patients - some degree of movement limitation • 25% cannot perform major activities of daily living • 11% knee OA need help with personal care • 14% require help with routine needs. • ~ 40% of adults with knee OA reported their health “poor” or “fair”. • 1999, knee OA - more than 13 days of lost work due to health problems
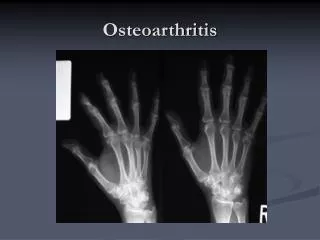
Excessive stress to entire joint • Articular (hyaline) cartilage • Synovial lining • Bone beneath cartilage • Ligaments • Diagnosed by X-Rays and symptoms • Joint space narrowing • Sclerosis (increased bone density) • Spurs, lipping
X-Rays of OA joints Normal knee Osteoarthritic knee
X-Rays don’t correlate well to pain • Decreased space: meniscus or articular cartilage • Cartilage: no nerves = no pain • X-Rays activity • Fear/anxiety = activity • Untreated OA lesions fared no worse • Widuckowski et al (2009) 2-4 cm lesions w/out tx no worse in 13 – 17 year follow-up • Surgical debridement of OA no better than physical therapy/medication • Risberg et al; Kirkley et al; Moseley et al
Risks for OA • Excess weight • For OA risk • Not for progression unless misalignments • Trauma, surgery, etc. • NO movement • Immobilization • Sedentary lifestyle • Repetitive, excessive twisting • Rapid impact activities • Excessive Joint flexibility • Misalignments/movement impairments
Articular cartilage • Hyaline cartilage – bluish, opalescent, glassy, homogenous • Thinner with age • No blood vessels / no nerves • Heals very slowly • No pain • 80% water-filled matrix • Must have dynamic (cyclic) loading to move nutrients in/damaged cells/waste products out.
Functions of articular cartilage • Absorb and distribute compressive forces • Like a gel bicycle seat • Lying down (~0 compressive force) - knee • Jumping (~24 x body weight) – knee • Flow of fluid through porous matrix, away from force. • Stiffer to higher loads • Shock absorption (deformation of cancellous bone most, then subchondral bone and slightly cartilage (1-3%) • Slippery • 500 to 2000 x slipperier than ice on ice. • Synovial fluid – consistency like egg white • Helps cartilage resist sliding forces
TENSILE FORCES Tensile stress-strain curve of articular cartilage
Compressive forces The non-linear response of articular cartilage to compressive force on fluid flow through the matrix
Types of physical stresses encountered by articular cartilage • Stretching (tensile) forces • Compressive forces • Sliding (shear) forces
Compressive loads • Short term • Eckstein et al Eckstein et al (2005) – • MRI before/after deep knee bends, squatting, walking, cycling – decreased thickness 5.0 to 8.8% • After 100 knee bends, return to original thickness took 90 minutes. • Long term changes • Inadequate load/immobilization • Jortikka et al (1997) – 11 weeks of immobilization PG in beagle knees – did not fully recover after 50 weeks or remobilization. • Hinterwimmer et al (2004) – 20 patients mean knee cartilage thickness after partial LE immobilization for ankle fx x 7 weeks. • Vanwanseele et al (2002) – after 2 years post-injury, spinal cord patients’ cartilage thickness patella 23%, medial tibia 25%, lateral tibia 19%.
Compression • Excess load = cartilage • Low compression ↑ synthesis; high decreased it. • Weak quadriceps (Youssef et al, 2009) saline or botox injected into quads. • Segal et al (2010) – weak quads correlated to JSN in women • Slemenda et al (1997)- each 10-lb/ft increase knee extensor strength = 20% knee OA • Mikesky et al (2006) – 221 older adults, strength vs ROM • Strength group showed slower rate of JSN at 30 months. • Excess weight increases load and risk • Felson et al in Framingham Study (1992), wt loss risk of knee OA • Sharma et al (2000) BMI correlated more with risk than progression except in bowed legs
Shear (sliding force) • Wong et al (2008) – cadaveric osteochondral cores subjected in vitro to shear with 15% compression. • More irregular surface had 5 x > shear than normal cartilage. • More irregular surface = > friction = more degradation with shear) • Shear more inflammation, production of degrading enzymes, etc. • Shear more common than excess compression with people over 60? • Clinically – patients often report more pain with movements that increase shear • Twisting and bending knees sideways • Less pain with movement impairment corrections
Causes of compression problems • Inadequate (rhythmic) compression • “I better not wear it out faster” • Sedentary lifestyle • Static postures • Prolonged standing • Excess compression • Excess body weight • High impact or rapid loading activities • Weak muscles (or muscles untrained for faster loads)
Causes of excessive shear • Activities which twist joints with compression • Skiing • Tennis • Dancing • Running with flexible knees • Poor movement patterns • Sit stand with knees in/out • Up/Down steps with hip/knees in/out • Poor body mechanics with activities
TISSUE RESPONSE TO PHYSICAL STRESS Optimum Health Healthier Cell death Cell death More physical stress
General advice about joint care • Avoid static postures – especially bad ones – move! • No pain, no gain = no brain. • Avoid joint noise if possible • Maintain adequate strength • Stretch muscles, not joints • Healthy weight • All joints need regular movement to feel their best. • If you can’t find comfort, seek help • Start with conservative care (physical therapy) • If no improvement in 6 – 8 visits, change therapists • Treat it as a mechanical problem
Feet are the foundation • Do not tolerate uncomfortable shoes – ever! • Maintain healthy weight • Alternate sport shoes each day • Shock absorption is slow to recover after compression • Choose activities that don’t hurt. • Walking is better than standing • Foot exercises?
Knees to last a lifetime • Healthy weight • Avoid unnecessary twisting • Biking? • Avoid breaststroke, scissor or frog kicks in swimming • Focus on alignment • Maintain strong legs and HIPS • Wear proper shoes
Hip, hip hooray! • IF flexible, avoid extreme stretches for hip • Avoid performing “splits,” race-walking, extreme yoga asanas that take hips back beyond neutral with pelvic • Maintain strong buttock and hip muscles • Avoid becoming “hamstring dominant” • Jogging worse than running • IF you have very stiff hips with OA, stretch the hips and strengthen them too
Spine pain • Seek help if: • Bowel/bladder problems • Decreased strength in lower extremity or upper extremity • Tingling/numbness in genital region • Sensory changes in both sides of UE or LE • Start with conservative care – proceed slowly on that route. • “But my MRI showed that…”
Spine: • Spine pain is a mechanical problem too • Posture • Exercise • Avoid heavy lifting • Never bend and lift or worse, bend, twist and lift • For heavy objects – the Raugh Method
Shoulders • Allow your shoulders to rise when you reach. • Lift in line with the shoulder blades • Don’t keep them down (for your neck too).