Download
1 / 1
10 likes | 93 Vues
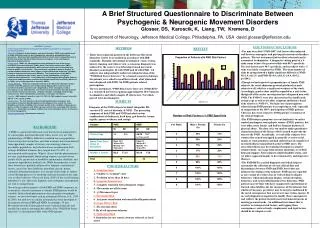
Did the patient have contact DURING THE LAST 18 MONTHS with a mammal capable of spreading rabies? 2. NOTE: Providers who have questions or concerns regarding application of this algorithm should contact their local Rabies Advisory Board for assistance. YES. NO Rabies PEP Indicated

E N D
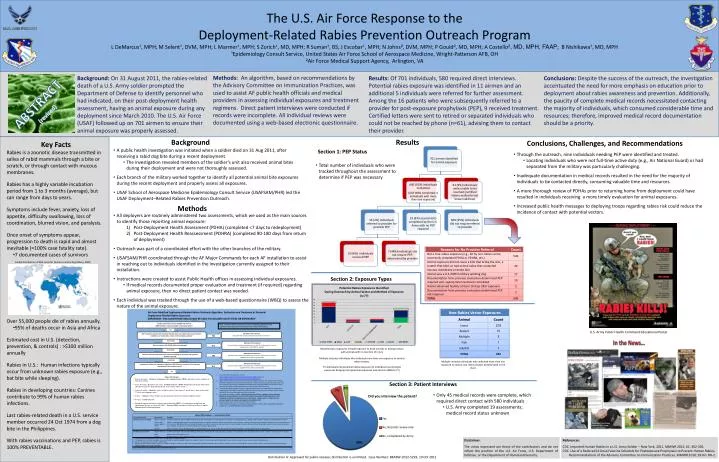
Did the patient have contact DURING THE LAST 18 MONTHS with a mammal capable of spreading rabies?2 NOTE: Providers who have questions or concerns regarding application of this algorithm should contact their local Rabies Advisory Board for assistance. YES NO Rabies PEP Indicated Document the incident and clinical assessment in AHLTA. Did the patient sustain a bite that broke the skin, have wet animal saliva contact mucous membranes or broken skin, or have a bat in sleeping quarters? NO YES/UNSURE NO Rabies PEP Indicated Document the incident and assessment in AHLTA. Code exposure³and use supplemental code E906 for dog bite. YES Was the animal a U.S./NATO military working dog? NO/UNSURE NO Rabies PEP Indicated Document the incident and assessment in AHLTA. Code exposure³and use supplemental E codes as appropriate. YES Was the animal directly observed for 10 days following the exposure and appeared healthy at day 10? NO/UNSURE NO Rabies PEP Indicated Document the incident and assessment in AHLTA. Code exposure³and use supplemental E codes as appropriate. Is appropriate rabiespost-exposure prophylaxis (PEP) (4 doses of vaccine) for this exposure documented in the medical record?4 YES NO Rabies PEP Indicated • 0 doses of vaccine: Administer both human rabies immunoglobulin (HRIG) and rabies vaccine regardless of time since incident. • 1 dose of vaccine: Restart vaccine series. No HRIG indicated. (HRIG should not be given more than 7 days after first vaccine dose if the patient already received some rabies vaccine.) • 2 doses of vaccine: Administer 2 doses of rabies vaccine, 7 days apart (3rd and 4th dose). Draw a titer on the 7th day to assess immune status.7 • 3 doses: Administer 1 dose of rabies vaccine and draw a titer for assessment of immune status.7 • 4+ doses: no PEP indicated. • Document exposure incident, assessment, and treatment in AHLTA. Use appropriate wound code and supplemental E codes, as well as code V04.5.3 Document HRIG and rabies vaccines in Air Force Complete Immunization Tracking Application. Background: On 31 August 2011, the rabies-related death of a U.S. Army soldier prompted the Department of Defense to identify personnel who had indicated, on their post-deployment health assessment, having an animal exposure during any deployment since March 2010. The U.S. Air Force (USAF) followed up on 701 airmen to ensure their animal exposure was properly assessed. Results: Of 701 individuals, 580 required direct interviews. Potential rabies exposure was identified in 11 airmen and an additional 5 individuals were referred for further assessment. Among the 16 patients who were subsequently referred to a provider for post-exposure prophylaxis (PEP), 9 received treatment. Certified letters were sent to retired or separated individuals who could not be reached by phone (n=61), advising them to contact their provider. Conclusions: Despite the success of the outreach, the investigation accentuated the need for more emphasis on education prior to deployment about rabies awareness and prevention. Additionally, the paucity of complete medical records necessitated contacting the majority of individuals, which consumed considerable time and resources; therefore, improved medical record documentation should be a priority. Methods: An algorithm, based on recommendations by the Advisory Committee on Immunization Practices, was used to assist AF public health officials and medical providers in assessing individual exposures and treatment regimens. Direct patient interviews were conducted if records were incomplete. All individual reviews were documented using a web-based electronic questionnaire. Background Results Conclusions, Challenges, and Recommendations • Key Facts • Rabies is a zoonotic disease transmitted in saliva of rabid mammals through a bite or scratch, or through contact with mucous membranes. • Rabies has a highly variable incubation period from 1 to 3 months (average), but can range from days to years. • Symptoms include fever, anxiety, loss of appetite, difficulty swallowing, loss of coordination, blurred vision, and paralysis. • Once onset of symptoms appear, progression to death is rapid and almost inevitable (≈100% case fatality rate). • 7 documented cases of survivors • Over 55,000 people die of rabies annually. • 95% of deaths occur in Asia and Africa • Estimated cost in U.S. (detection, prevention, & controls) : >$300 million annually • Rabies in U.S.: Human infections typically occur from unknown rabies exposure (e.g., bat bite while sleeping). • Rabies in developing countries: Canines contribute to 99% of human rabies infections. • Last rabies-related death in a U.S. service member occurred 24 Oct 1974 from a dog bite in the Philippines. • With rabies vaccinations and PEP, rabies is 100% PREVENTABLE. The U.S. Air Force Response to the Deployment-Related Rabies Prevention Outreach ProgramL DeMarcus¹, MPH; M Selent¹, DVM, MPH; L Marmer¹, MPH; S Zorich¹, MD, MPH; R Suman¹, BS; J Escobar¹, MPH; N Johns², DVM, MPH; P Gould², MD, MPH; A Costello², MD, MPH, FAAP; B Nishikawa¹, MD, MPH¹Epidemiology Consult Service, United States Air Force School of Aerospace Medicine, Wright-Patterson AFB, OH²Air Force Medical Support Agency, Arlington, VA • A public health investigation was initiated when a soldier died on 31 Aug 2011, after receiving a rabid dog bite during a recent deployment. • The investigation revealed members of the soldier’s unit also received animal bites during their deployment and were not thoroughly assessed. • Each branch of the military worked together to identify all potential animal bite exposures during the recent deployment and properly assess all exposures. • USAF School of Aerospace Medicine Epidemiology Consult Service (USAFSAM/PHR) led the USAF Deployment–Related Rabies Prevention Outreach. Section 1: PEP Status • Through the outreach, nine individuals needing PEP were identified and treated. • Locating individuals who were not full-time active duty (e.g., Air National Guard) or had separated from the military was particularly challenging. • Inadequate documentation in medical records resulted in the need for the majority of individuals to be contacted directly, consuming valuable time and resources. • A more thorough review of PDHAs prior to returning home from deployment could have resulted in individuals receiving a more timely evaluation for animal exposures. • Increased public health messages to deploying troops regarding rabies risk could reduce the incidence of contact with potential vectors. • Total number of individuals who were tracked throughout the assessment to determine if PEP was necessary Methods • All deployers are routinely administered two assessments, which we used as the main sources to identify those reporting animal exposure: • Post-Deployment Health Assessment (PDHA) (completed <7 days to redeployment) • Post-Deployment Health Reassessment (PDHRA) (completed 90-180 days from return of deployment) • Outreach was part of a coordinated effort with the other branches of the military. • USAFSAM/PHR coordinated through the AF Major Commands for each AF installation to assist in reaching out to individuals identified in the investigation currently assigned to their installation. • Instructions were created to assist Public Health offices in assessing individual exposures. • If medical records documented proper evaluation and treatment (if required) regarding animal exposure, then no direct patient contact was needed. • Each individual was tracked through the use of a web-based questionnaire (WBQ) to assess the nature of the animal exposure. ABSTRACT (revised) Global Distribution of Risk Level for Humans Contracting Rabies, 2009 Section 2: Exposure Types Air Force Modified Deployment-Related Rabies Outbreak Algorithm: Evaluation and Treatment of Potential Deployment-Related Rabies Exposures IMPORTANT: THIS ALGORITHM SHOULD NOT BE USED TO EVALUATE ACUTE BITES OR EXPOSURES1 U.S. Army Public Health Command Educational Poster In the News… • Miscellaneous exposures include exposure to dead animals or having contact with animals with no mention of injury • Multiple includes individuals who indicated more than one exposure to various rabies vectors. • 73 individuals had potential rabies exposures (4 individuals had multiple exposures bringing total potential exposures entered into WBQ to 77) • Multiple includes individuals who indicated more than one exposure to various non-rabies vectors already listed in the chart. • For acute bites and exposures, refer to http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5703a1.htmand http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5902a1.htm. • Dogs, cats, bats, raccoons, skunks, ferrets, foxes, mongooses, jackals, and other medium‐to‐large mammals. Rodents are not reservoirs of rabies virus. Small rodents (e.g., squirrels, chipmunks, rats, mice, hamsters, guinea pigs, and gerbils) and lagomorphs (including rabbits and hares) are rarely infected with rabies and have not been known to transmit rabies to humans. • Use codes 870.0‐897.7 (wound, open) or 910‐919 (superficial injury codes) with the appropriate supplemental code E906 for dog bite or E906.5 for injuries due to monkey or other animal. Include code V04.5 for animal bite requiring rabies vaccination. • See protocols on page 2. Note: as these exposures are historic, consider 4 doses of human diploid cell vaccine (HDCV) or purified chick embryo cell vaccine (PCECV) adequate for PEP, regardless of whether the patient was on antimalarials. Patients with 3 or fewer doses of vaccine should be contacted and brought in for additional PEP. • If vaccine doses were missed, restart the vaccine series. • PCECV should not be given to individuals with egg allergies. HDCV is safe in egg‐allergic individuals. • If titer <1:5, call USAFSAM for further guidance. Section 3: Patient Interviews • Only 45 medical records were complete, which required direct contact with 580 individuals • U.S. Army completed 19 assessments; medical record status unknown Disclaimer: The views expressed are those of the contributors and do not reflect the position of the U.S. Air Force, U.S. Department of Defense, or the Department of Homeland Security. References: CDC. Imported Human Rabies in a U.S. Army Soldier – New York, 2011. MMWR 2012; 61: 302-305. CDC. Use of a Reduced (4-Dose) Vaccine Schedule for Postexposure Prophylaxis to Prevent Human Rabies. Recommendations of the Advisory Committee on Immunization Practices. MMWR 2010; 59:No. RR-2. Distribution A: Approved for public release; distribution is unlimited. Case Number: 88ABW-2012-5293, 10 Oct 2012