Download
1 / 37
680 likes | 3.8k Vues
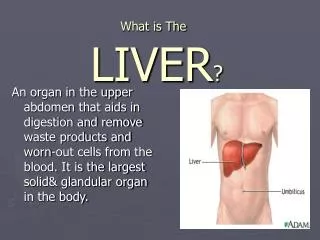
An organ in the upper abdomen that aids in digestion and remove waste products and worn-out cells from the blood. It is the largest solid& glandular organ in the body. . What is The LIVER ?. What is the blood supply of the liver?.

E N D
An organ in the upper abdomen that aids in digestion and remove waste products and worn-out cells from the blood. It is the largest solid& glandular organ in the body. What is TheLIVER?
What is the blood supply of the liver? Liver has a dual blood supply; portal vein(75%) & hepatic artery (25%),The hepatic veins are responsible for drainage of filtered blood from the liver into the IVC.
Morphological anatomy is based on the external appearance of the liver and does not show the internal features of vessels and biliary ducts branching, which are important in hepatic surgery. Functional anatomy divides the liver into eight functionally independent segments. Each segment has its own vascular inflow, outflow and biliary drainage What about Liver anatomy??Liver anatomy can be described using two different aspects
What’s the significance of functional anatomy!? In order to perform segmental or subsegmental resection of the liver, the surgeon must know exactly which parts of the liver are diseased so that vascular supply and venous and biliary drainage can be preserved& also Because of this division into self-contained units, each segment can be resected without damaging those remaining.
There are many anatomical and functional descriptions of the liver anatomy such as Classical Anatomy &Bismuth's classification however (Couinaud classification) is the most commonly used classification.
Couinaud classification • The Couinaud classification of liver anatomy divides the liver into eight functionally independent segments. • Each segment has its own vascular inflow (hepatic artery & portal vein), outflow (hepatic vein) and biliary drainage
How are the segments spatially separated? • Right hepatic veindivides the right lobe into anterior and posterior segments (segment 6& 7 usually not visulaized at the frontal view). • Middle hepatic veindivides the liver into right and left lobes (or right and left hemiliver). This plane runs from the inferior vena cava to thegallbladder fossa(Cantlie's line) • Left hepatic veindivides the left lobe into a medial and lateral part. • Portal veindivides the liver into upper & lower segments.
What are liver segments?? • Couinaud's numbering system: 1-Caudate Lobe (posteriorly) 2-Left Superior Lateral segment 3-Left Inferior Lateral segment 4a-Left Superior Medial segment 4b-Left Inferior Medial segment 5-Right Inferior Anterior segment 6-Right Inferior Postrior segment 7-Right Superior Postrior segment 8-Right Superior Anterior segment
How can you interpret this classification at the transverse images? • Imagine the liver is sliced at 4 levels & then analyze the previously mentioned liver segments at each level:
This figure is a transverse image through the superior liver segments, that are divided by the hepatic veins.
This figure shows transverse image at the level of the left portal vein.At this level the left portal vein divides the left lobe of liver into superior segments (2 and 4A) and inferior segments (3 and 4B).
The image on the left is at the level of right portal vein. At this level right portal vein divides the right lobe of the liver into superior segments (7 and 8) and the inferior segments (5 and 6).The level of right portal vein is inferior to the level of left portal vein
below the level of the main portal vein: The gallbladder separates segment(V) from segment (IVB). The ligamentum teres divides segment(IVB) and (III) segments.
Above the level of this image segments from left to right are7,8,4,2 Below & at this level segments from left to right are 6,5,4,3 TO REMEMBER Level of splenic v&main portlv
Modalities of Liver Imaging • Ultrasound • CT • MRI • Nuclear Medicine
Ultrasound • Is the first and the most commonly obtained method of examination in patients with RUQ pains, abnormal LFTs, or suspected liver masses. • Is a noninvasive and excellent screening tool. • Used to evaluate the presence of bile duct obstruction and gallstones as well as to distinguish a solid lesion from a cystic one. • Has low sensitivity and high false negative rate for detection of liver metastases.
Ultrasound Doppler imaging can be very helpful in identifying vascular abnormalities, i.e. patency of hepatic vessels, portal vein, and IVC as well as flow direction in these vessels. Flow in the portal vein and hepatic arteries are hepatopedal (toward the liver) while flow in hepatic veins and hepatic ducts are hepatofugal (away from the liver).
CT • Uses X-ray to acquire data that can be displayed in axial, coronal, and sagittal planes. • I.V. iodinated contrast is commonly used in liver imaging to demonstrate any abnormal enhancement of a hepatic lesion and to show vascular structures. • An I.V. bolus of 100 to 150 ml of iodinated contrast is often used. The contrast agent is injected into veins, travels to the heart, aorta, celiac trunk, hepatic arteries, liver parenchyma and mixes with blood in portal veins drained into venules and then hepatic veins and then out to the IVC.
the hepatic enhancement can be divided into 3 phases: 1-Arterial phase (when the contrast just fills up the aorta and the main hepatic arterial structures),kidneys also show corticomedullary differentiation 2-Portal venousphase (when the contrast disperses into the liver parenchyma (liver brighten) and mixes with portal blood (portal v brighten) 3-Equilibrium phase (Delayed phase) (when the contrast further scatters in the parenchyma and drains out the hepatic veins and also be seen in the renal collecting system).
When searching for hypervascular lesions, such as hepatoma or metastastic disease, a three-phase technique often should be used: non-contrast phase, arterial phase, and portal venous phase. • The appropriate delay times for scanning in the arterial phase and portal venous phase for a 2-3 ml/sec injection are 25 seconds and 70 seconds, respectively. • The rationale behind this technique is that primary and secondary malignancies of the liver typically have hepatic arterial supply, thus will enhance during the arterial phase, whereas benign entities and normal liver parenchyma have primarily portal venous supply, therefore, will enhance during portal-venous phase of I.V. contrast.
Rapid Wash outNote here also the lesion at the non contrast image then early enhancement at the arterial phase and rapid wash out a the portal phase (yellow arrows)very characterstic of HCC Progressive fill in (note the lesion at non enhanced image,then peripheral enhancement in arterial phase &further central filling at portal phase then total enhancement at the delayed image) Very characterstic of hemangioma
MRI • Indications for Liver MRI 1- Patients are allergic to iodinated contrast agents. 2-Lesion detection & characterization . 3-Anatomic location . 4-Hepatic vascular patency . 5-Biliary duct system.
MRI has many advantages over CT: High soft tissue contrast resolution (can see smaller lesions), Multiple sequences, Multiplanar capability, MRA, MRV, MRCP, No radiation, no iodinated contrast·etc.
However, MRI is similar to CT in that it has the same dynamic multiphase contrast enhancement capability. • MRI can be helpful in the characterization of a small (< 2 cm) benign hemangioma that is equivocal on CT.
A wide range of MRI sequences is available for liver imaging thanks to the numerous manipulations of field strength, pulse sequence, and interdependent sequence parameters which can affect image quality. Since there is little agreement on the best technique, MRI sequences are often unique to the institution. At UVa, we use the following: • Breath hold T1 spoiled gradient echo (In phase and out of phase): can be used to detect fatty liver, fat in HCC, focal fatty infiltration/sparing, adrenal adenomas. • Breath Hold T2: can be used to evaluate hemangiomas and cysts. • Turbo spin echo with fat sat or STIR • HASTE -Half Fourier acquisition single shot turbo spin echo • Dynamic Gad T1 (Arterial, portal venous, delayed, timing bolus, or smart prep): can be used to characterize hypervascular lesions.
For most techniques, the intensity of normal liver parenchyma is the same as or slightly higher than that of adjacent muscle. Normally, the liver should be brighter than (hyperintense to) the spleen on T1-weighted images and darker than (hypointense to) the spleen on T2-weighted images.
Developmental Anomalies and Anatomic Variants of the liver Embryonic development of the liver, pancreas, extrahepatic biliary apparatus, and duodenum.
Agenesis of the right hepatic lobe. A. CT reveals agenesis of the right lobe of the liver with compensatory hypertrophy of the left lobe
Agenesis of the left hepatic lobe. CT shows tongue like projection (arrow) of caudate lobe at the upper image.
Diaphragmatic invagination As a result of invagination of diaphragmatic slips along the superior aspect of the liver, pseudoaccessory fissures are formed.
Accessory fissure in the under surface of the liver. The accessory fissure in the right lobe
Sliver of liver. The T2-weighted image of the upper abdomen reveals leftward lateral extension of the left lobe of the liver ,which appears as a crescentic low-intensity structure wrapping around the lateral aspect of the spleen. If the communication is not seen, it can mimic abnormal structure lateral to the spleen. This occasionally is the case in abdominal ultrasound.
Papillary process of the caudate lobe. The contrast-enhanced CT scan shows medial and posterior extension of the papillary process near the head of the pancreas mimicking a mass lesion.
Papillary and caudate process pseudomass. The T1-weighted fat-suppression images reveal medial extension of the papillary process near the head of the pancreas. Notice the signal characteristics of this mass being similar to the remainder of the liver and not of the pancreas.
Riedel's lobe. A. Topogram from the patient's CT scan displays an elongated inferior extension of the right lobe of the liver (arrows) characteristic of a Reidel lobe