Download
1 / 60
600 likes | 896 Vues
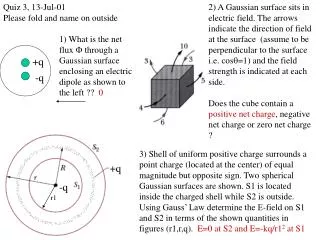
Surface Ablation: Indications and Management. Eric E. Polk, OD, FAAO Adjunct Assistant Professor St. Louis, MO. PRK Outline. Types of Procedures Indications Management Complications Contraindications. Surface Ablation: On the Rebound?. LASIK or Surface Ablation?. LASIK Advantages

E N D
Surface Ablation: Indications and Management Eric E. Polk, OD, FAAO Adjunct Assistant Professor St. Louis, MO
PRK Outline • Types of Procedures • Indications • Management • Complications • Contraindications
LASIK or Surface Ablation? • LASIK Advantages • Great vision • Quick healing time • Minimal discomfort • Little inconvenience • Patients want all of this and they want it done safely
LASIK Disadvantages • LASIK Disadvantages • Flap complications • Buttonhole flap • Interface complications • DLK, Epithelial Ingrowth, .. • Displaced flaps • More difficult to perform • Compromises the central corneal thickness • Keratectasia
Advantages of Surface Ablation • Preserves corneal thickness • No Interface • Easier learning curve • Better Visual Acuity? • No Flap • Flap Displacements
Advantages of Surface Ablation • Recommended for naval pilots • Proven long term results • Rajan MS, et al. A long-term study of PRK: 12-year follow-up. Ophthalmology 2004; May: 5-19.
Disadvantages of PRK • Longer visual recovery • More discomfort • Risk of haze • Not as well known • Unilateral surgery • Anisometropia, aniseikonia
Types of Surface Ablation • PRK • LASEK • Epithelial LASIK
PRK Surgery • First PRK surgery done in 1986 • Also called advanced surface ablation • Epithelium is removed and laser is applied
Epithelial Removal • Different techniques of epi removal • Brush • Alcohol • PTK • Scrape
LASEK • Laser Epithelial Keratomileusis • Laser-assisted subepithelial keratectomy • First introduced by Dr. Camellin in 1999 • A well filled with 20% alcohol is applied to the cornea for 20 to 40 seconds
LASEK • Epithelium is moved to the edge of the cornea • Have to be careful not to tear epi on removal
LASEK • Epithelium is reapplied to the cornea and a bandage CL is applied • Epithelial flap will re-adhere to cornea within next 4-5 days
PRK VS LASEK • Is there an advantage? • Camellin, M. LASEK for myopia. Journal of Refractive Surg 2003;19:666-70. • Proposed advantages of LASEK: • Less pain • Quicker visual recovery • Less haze
PRK versus LASEK • My Experience • PRK and LASEK seem to give similar results • Haze, discomfort and healing is the same • Some LASEK patients have EBMD appearance to the cornea
Epithelial-LASIK • Introduced by Ioannis Pallikaris, MD • Epithelial microkeratome mechanically creates an epithelial flap Centurion SES
Epi-LASIK • Mechanical separation of epithelium from Bowman’s membrane. • Epithelial flap is folded back and the laser ablation is applied • Systems use metal blades, PMMA plastic or high pressured water
Basement Membrane Cleavage Plane = 1 micron in dia. Bowman’s Layer Anterior Stroma Histology: Donor Cornea / B. Jackson, M.D., Ottawa, Canada
Proposed Advantages • Less discomfort • Quicker visual recovery • Less haze • Cells are more viable • Epithelial flap may inhibit cytokine release • Dai J, et al. One-year outcomes of epi-LASIK for myopia. J Refract Surg. 2006;22:589-95.
EPI-LASIK Disadvantages • Drawbacks • Anecdotal case reports of abnormal flaps and stripping of Bowman’s layer • Reports of epithelium growing under epithelial flap • Learning curve • Cost
Indications for Surface Ablation • Thin Corneas • Steep Corneas/ Flat Corneas • Risk with microkeratome • Re-treatments over LASIK/ RK • EBMD
Keratectasia • Number one reason we recommend surface ablation • Very uncommon complication • Incidence • 1/5000 to 1/10,000 Cases • Cornea bows forward following laser surgery • Symptoms • Blurred Vision that is not correctable by enhancement surgery • Diplopia • Decreased Night Vision • Ghost Imaging
Which patients are at higher risk for developing ectasia? • Two types of patients 1) Thin residual stromal beds • Corneal thickness following refractive surgery 2)Patients who have a predisposition for developing ectasia • Keratoconus • Forme fruste keratoconus • Pellucid marginal degeneration
Case Report • 22 y/o white male • -6.00 -1.00 X 180 OU • Pachymetry: 545 OU • Slit Lamp exam: WNL • Recommend PRK Surgery
Indications for PRK Risk of Buttonhole flap • Microkeratome blade travels anterior and enters the epithelium/ bowman’s complex. • Much lower risk with IntraLase • Risk factors?
Indications for PRK Surgery: Retreat Surgery • Surface ablation over previous RK surgery • Mitomycin C • Surface ablation over previous LASIK surgery • Mitomycin C
PRK Retreat over RK • Better option then LASIK retreat • Will not stop fluctuations to vision • Risk for haze formation • Mitomycin C • Results are a little more variable then primary LASIK
PRK Retreats over LASIK Flaps • PRK retreat over LASIK flap • Flaps with epithelial ingrowth • Flaps that are difficult to lift (old flaps) • Thin Post-operative corneas • Risk of corneal haze
PRK Over LASIK Flap • 35 Year old patient wants retreat surgery • Pre-op Hx • -6.00 Myope • 500 Pre-operative pachymetry • Intra-operative Pachymetry revealed 150 micron flap • Post-op • -1.00 Myope • Pachymetry: 400 Microns • “Wants better Distance Vision” 500 -150 Flap -100 Ablation =250
Indications: EBMD • Epithelial basement membrane dystrophy • 5% of the population over the age of 50 • Typically asymptomatic
Indications: EBMD • EBMD increases risk of abrasion during LASIK • Abrasions increase risk of: • Epithelial ingrowth • Diffuse lamellar keratitis • Irregular astigmatism • Prolonged visual recovery
Absolute Contraindications for Surface Ablation • High RX • Above ~-9.00 • Keratoconus • Pellucid Marginal Degeneration • Unrealistic expectations
Concerns for Surface Ablation • Keloid Formers • Risk of Haze • Glaucoma Patients • Risk of IOP spike
Management of Surface Ablation Procedures • Manage Epithelial Healing • Bandage CL • Manage Haze • Manage Visual Recovery
Epithelial Healing • Similar to managing a large abrasion • Bandage contact lens • Antibiotic • Epithelial healing takes 4-5 days Dr.Camellin
Day 1 Post-Op • Check visual acuity • Ranges from 20/30 to 20/200 • VA may decrease in next 2 days • Slit lamp exam • Centered CL • Check for signs of infection
Bandage CL • High water, oxygen permeable. • Ciba Focus Night and Day • Bausch and Lomb Pure Vision • AcuvueOasys
5 Day Post-Op • Check vision • Range of 20/25 to 20/80 • Remove CL • Epithelium need not be pristine • Comfort of patient • Extended use of CL increases risk of Infection
Eye drop Regimen • Non-steroidal QID X 4 Days • Acular, Xibrom • Decreases eye pain • Antibiotic QID X 7 Days • Zymar, Vigamox • Infection • Mild Steroid: QID X 1st Month • Fluoromethelone 1% • Haze, regression
Steroid Prevents • Regression • Under correction • Maintain FML Drops • Over correction • Decrease FML Drops • Haze • Greater haze • Maintain FML Drops • Example:1 month post-op PRK patient is myopic and has mild haze: • Continue steroid
Surface Ablation Informed Consent • Prolonged Visual Recovery • Unilateral Surgery • Discomfort • Infection • Haze
Prolonged Visual Recovery • Patients need to be prepared for longer vision recovery • Five days of blurry vision with bandage CL • 2 weeks before epithelium is smooth enough for comfortable vision (20/30)
Prolonged Visual Recovery • Six months before you reach optimal vision. • Six month time period before considering enhancement.
Unilateral Surgery • Recommend one eye at a time for most patients • Bilateral for patients who can take time off from work (5-7 Days) • Typically 2 weeks apart • Aniseikonia/ Anisometropia • Recommend CL wear in un-operated eye
Pain Management • Chilled BSS during surgery • NSAID eyedrops • Tylenol with codeine • Some doctors recommend • Diluted proparicaine • Neurontin • Indicated for the management of postherpetic neuralgia
Regression • May occur months after surgery. • Steroid eye drops may help prevent regression. • Risk factors • Higher RX >-6.00/+4.00 • Sunlight • Haze
IOP Spikes • Prolonged steroid usage • Use FML versus Pred-Forte • May require concomitant use of glaucoma agent and steroid • Check IOP on follow-up appointments
Infection • Incidence 1/1000 with PRK • 1/5,000 with LASIK • Bandage CL • Open Wound • Steroid Drops