Download
1 / 35
380 likes | 1.42k Vues
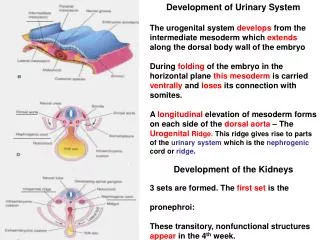
Development of the Urinary System. Urinary and genital systems are closely associated Both develop from intermediate mesoderm 7 th - 28 th somite level Nephrogenic mass (cord) Dorsal side of coelom each cord produces a bulge into the coelom called the urogenital ridge Urinogenital Ridge

E N D
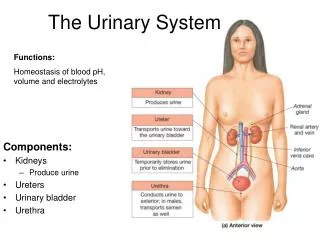
Development of the Urinary System • Urinary and genital systems are closely associated • Both develop from intermediate mesoderm • 7th- 28th somite level • Nephrogenic mass (cord) • Dorsal side of coelom each cord produces a bulge into the coelom called the urogenital ridge • Urinogenital Ridge • Form the urinary and genital structures • Nephrogenic tissue from 7-14th somite breaks up into segments called nephrotomes
Intermediate Mesoderm • Cervical region • Loses contact with the somite • Forms nephrotomes which acquire a lumen and open medially into the intra-embryonic coelom • Caudal growth unite and form longitudinal duct • Branches off dorsal aorta form glomeruli (ext & int) • Thoracic, lumbar, sacral regions • Loses contract with coelomic cavity • Ext glomeruli fail to develop • Segmentation disappears (nephrogenic cord) • 2 or more excretory tubules per prior segment
Urinary Tubules • Associated with a vascular tuft = glomerulus • Open tubules = external glomerulus • One end opens into the coelom • Other end opens into the collecting duct • Closed tubules = internal glomerulus • Open only into the collecting ducts
Formation of 3 kidney systems • Pronephros (simplest & most primitive) • 7-10 solid or tubular arranged cell groups in the cervical region (head kidney) • Gone by the end of the 4th week • Mesonephros (intermediate-more advanced) • Appear during regression of pronephros • 10-26th somite level • Metanephros (permanent kidney) • Begins to develop early in 5th week, functions by the 11th week
Mesonephros • Tubules develop from nephrogenic cord (NC) • Opens into the excretory/mesonephric duct • Gone by week 10 in females, in males some tubules persist & become vas deferens • Approximately 38 pairs of closed tubules • S shaped bend • Surrounds internal glomerulus • Mesonephric duct develops laterally from NC & extends from 8th somite to urinogenital sinus
Metanephros • Nephrons/tubules develop from nephrogenic mass (26th-28th somite level) • Located lateral to mesonephric duct • Internal dense layer which forms tubules/nephrons • Outer loose layer forms connective tissue capsul • Duct system derived from ureteric bud • Ureter, renal pelvis, calyces, collecting ducts • Ureteric bud elongates and makes contact with nephrogenic mass which surrounds bud like a cap • Tubules are closed (internal glomerulus) • Migrate from pelvis to abdomen as fetus grows • Blood supply from aorta changes as ascent occurs • Becomes functional in second ½ of pregnancy
Production of urine by fetus • Fetal urine mixes with amniotic fluid • Amniotic fluid enters fetal intestinal tract where it is absorbed into bloodstream • From the bloodstream to the placenta which transfers metabolic waste to the mother • Fetal kidneys are not necessary for exchange of waste products • Bilateral renal agenesis • 40% stillborn, live birth; death within hours-days
Cloaca • Caudal end of the hindgut (dilated) • In 3 week old embryo the hindgut ends blindly at the cloacal membrane • Blind end = cloaca • Allantois and mesonephric ducts open into cloaca • Cloaca is latin for _________
Urinary Bladder • During 4th to 7th week cloaca subdivided • Posterior portion = anorectal canal • Anterior portion = primitive urogenital sinus • Bladder is formed from primitive urogenital sinus • Bladder is upper and largest part of urogenital sinus • Initially bladder is continuous with the allantois • Allantois lumen obilterated & urachus formed connecting apex of bladder with umblicus • In adult urachus = median umbilical ligament • Ureter is outgrowth of mesonephric duct • Terminal ends of mesonephric ducts become part of bladder wall • Ureter obtains separate entrance into bladder with time
Congenital Malformations • Renal agenesis • Unilateral • Bilateral • Renal hypoplasia • Congenital cystic kidneys • Types 1 -5 • Horseshoe (fused) kidneys • Wilms tumor
Renal Agenesis • Absence of kidneys • Unilateral (compatible with life) • Affects 1 in every 800-1500 people • May occasionally present with genitalia anomolies • Trisomy of 18 • Addition or partial trisomy of 13 • Prenatal rubella infection • Bilateral (incompatible with life) • 40% stillborn • Of those born alive 95% die within 24 hours of birth • Potter syndrome and associated oligohydramnios
Renal hypoplasia • Incomplete development of kidneys • Unilateral (compatible with life) • Bilateral (incompatible with life) if condition is severe • Kidneys are small • Decreased functional parenchyma
Congenital cystic kidneys • Type 1 • Polycystic kidneys found in infants • Bilateral and results in early death • AKA giant or sponge kidneys • Large renal pelvis and calyces • Type 2 • Cysts are variable in size and shape • Usually unilateral • Affected kidney non functional
Congenital cystic kidneys (cont.) • Type 3 • Affected kidneys contain both normal and abnormal tissue • Both kidneys involved • Autosomal dominant gene • Trisomy of 13-15, 18, 21, 22 • Type 4 • Caused by urethral obstruction • If severe early death • Type 5 • Manifests during adult life, death by 50. • Autosomal dominant
Horseshoe (fused) kidney • Fusion of two kidneys at their lower end • Tissue that connects kidneys = isthmus • 1:400 • Trisomy 13-15; 18, 21, Turner’s syndrome, mosaicism • In rats horseshoe kidney can be produced experimentally by creating vitamin A deficiency
Wilms Tumor • Renal tumor of children • Characterized by rapid growth and early metastasis • Mesodermal origin • Metanephric tissue that have failed to differentiate into normal kidney tissue
Development of the reproductive system • Makes its appearance during 5th & 6th week • Indifferent stage-sex cannot be determined • Gonads (testes & ovaries) develop from • Coelomic epithelium • Inner mesenchyme tissue • Primordial germ cells • Thickening of ventromedial surface of urogenital ridge forming genital ridge
Genital ridge • Covered by coelomic epithelium • Primary sex cords • Grow into underlying mesenchyme • Inner mass is composed of mesenchyme • Outer layer called cortex • Inner layer called medulla • Males- medulla differentiates, cortex regresses • Females-cortex develops, medulla regresses
Primordial Germ Cells (PGC) • Differentiate in the neck of the yolk sac • Early in the 4th week • Migrate to genital ridge • Amoeboid movement • By end of 6th week the PGC become incorporated into the primary sex cords • migration of primordial germ cells
Development of testes • Primary sex cords of testes containing the primordial germ cells = testes cords • Well defined cords within the medulla • Contain two types of cells • Epithelial cells Sertoli cells • Primordial germ cells spermatoblasts • development of testes • Testes cords remain solid until puberty • Canalize to form seminiferous tubules (ST), tubuli recti, rete testis • ST seperated from each other by mesenchyme that gives rise to interstitial cells (Cells of Leydig)
Development of the Ovaries • Primary sex cords are not well defined • Extend into the medulla but later dissappear • PGC migrate near the cortex (surface epithelium • Forms cortical cords • At about 16th week cortical cords break up into isolated clusters called primordial follicles • development of ovary
Primordial Follicles • Follicle contains • Ooblast (oogonium) • Derived from the primordial germ cell • Undergoes mitosis during fetal life • Results in development of primary oocyte • A number of follicular cells • Derived from the cortical cords • Each primary oocyte surrounded by follicular cells = primary follicle • follicular development
Development of Genital Ducts • Indifferent stage • Both male and female genital ducts present • Male develop from mesonephric/wolffian ducts • Female develop from paramesonephric/mullerian duct • Undifferentiated gonad • Males:Mesonephric ducts form epididymis, ductus deferens, ejaculatory duct • Cranial mesonephric tubules efferent ducts • Open into epididymis • Process begins about the 3rd month
Development of Genital Ducts • Females: Paramesonephric duct/Mullerian duct develops on each side of the body • Longitudinal invagination of coelomic epithelium on the lateral surface of mesonephros • Ducts open into coelom • Runs along side of mesonephric duct • Fuse at caudal end • Y shaped uterovaginal complex uterus & vagina • uterovaginal complex
Fetal testes • Produce androgens • Stimulate development of mesonephric ducts • Suppress formation of paramesonephric ducts • If testes fail to develop or removed • Paramesonephric ducts will develop • Removal of fetal ovaries • Has no effect on fetal sexual development
Development of external genitalia • Indifferent stage • Genital tubercle • Develops at upper end of cloacal membrane • Elongates to form the Phallus • Labioscrotal swellings appear • Urogenital folds appear • Cloacal membrane divided into two • Development of urorectal septum • Upper urogenital membrane • Lower anal membrane • These membranes rupture around week 7 forming urogenital and anal openings
Development of external genitalia • Male genitalia • Phallus elongates to form the penis • Enlongation pulls the urogenital folds together • When folds start to fuse they enclose the urethra • Urethral opening moves progressively towards end of penis • Labioscrotal swellings fuse forming scrotum • Female genitalia • Phallus becomes clitoris (relatively small) • Urogenital folds do not fuse labia minora • Labioscrotal fuse only at ends labia majora
Accessory sex glands • Male • Highly developed • Seminal vesicles • Prostate • Bulbourethral glands • Female • Minimal • Major vestibular glands (homologous to bulbouretharal glands in male)
Congenital Malformations • Ovarian hypoplasia • Pure gonadal dysgenesis • Testicular feminization syndrome • Hermaphroditism • true • Female pseudohermaphroditism • Male pseudohermaphroditism • Hypospadias • Epispadia
Ovarian hypoplasia • Small overies • Poor breast development • Small uterus • Found in Turner’s syndrome • Incomplete or partial X chromasome • Can be unilateral or bilateral • Unilateral fertile • Bilateral infertile
Pure Gonadal Dysgenesis • Normal karyotypes (46, XX or 46, XY) • Primordial germ cells do not migrate from the yolk sac • No development of the ovaries or testes
Testicular Feminization Syndrome • Occurs at rate of 1:50,000 • Appears to be a normal female despite the presence of testes in either abdomen or inguinal region • Testes produce normal levels of testosterone • Tissues unresponsive to androgens • External genitalia are normal • Shallow blind ending vagina
Hermaphroditism • True hermphrodite • Both ovaries and testicular tissue present • Masculine form • Feminine form • Intermediate form (more common) • 46, XX/ 46, XY or 46, XX/ 47, XXY
Hermaphroditism • Female pseudohermaphroditism (46, XX) • AKA congenital adrenogenital syndrome • Masculinization due to high level of androgens from adrenal cortex • Male pseudohermaphroditism • Testes and ambiguous female genitalia • Many types, most common is of unknown etiology • Often considered females at a young age because penis is absent • Raised as girls until puberty when male secondary sex characteristics appear via endocrine activities of testes
Hypospadia/Epispadia • Hypospadia • Urethral opening on the ventral side of the penis (failure to completely cannulate) • Glandular and Penile (80%) • Penoscotal and perineal (20%) • Classification based on the location of the urethral orifice • Epispadia • Urethral opening on the dorsal side of the penis