Download
1 / 20
200 likes | 656 Vues
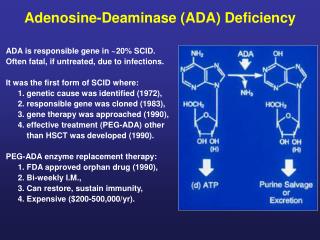
Adenosine Induced Bronchospasm . Anes R3 鄭淳心. Case report:. 病歷號 : 4129285 姓名 : 張德 X 身高 : 169.5cm 體重 : 60 Kgw 年齡 : 62 y/o 性別 : M 科別 : SURG-chest. Lab.data 1:. WBC 10.1 K/μL RBC 5.06 M/μL HB 14.0 g/dL HCT 44.2 % PLT186.0 K/μL Alb 3.9 g/dL TP 6.1 g/dL PT, PTT :WNL.

E N D
Adenosine Induced Bronchospasm Anes R3 鄭淳心
Case report: 病歷號 : 4129285 姓名 : 張德X 身高 : 169.5cm 體重 : 60 Kgw 年齡 : 62 y/o 性別 : M 科別 : SURG-chest
Lab.data 1: • WBC 10.1 K/μL • RBC 5.06 M/μL • HB 14.0 g/dL • HCT 44.2 % • PLT186.0 K/μL • Alb 3.9 g/dL • TP 6.1 g/dL • PT, PTT :WNL
Lab. Data2: • UN12.2 mg/dL • CRE 0.8 mg/dL • UA 4.9 mg/dL • Na 147.0 mmol/L • K 4.0 mmol/L • Cl 105.0 mmol/L • Ca 2.34 mmol/L • T-CHO 233.0 mg/dL
EKG: NORMAL SINUS RHYTHM, RATE 84 -- normal P axis, PR, rate & rhythm
Imaging study: • CXR shows normal heart size with increased lung markings. Mild fibrotic change is found at bil. lung fields with emphysematous change at lower lungs. COPD is suspected • HRCT of chest for the pulmonary bullous disease:1. multiple large bullae formation in the RML (lower lung fields, at the anterior aspect).2. diffuse pneumatoceles in both lung fields due to COPD with emphysematous change.3. nonspecific small nodes in the mediastinum.4. bilateral renal cysts.
Impression : COPD with emphysema; large bullae in the RML. • Surgical planning: VATS for Wedge resection
Induction for anesthesia: • Pre-oxygenation • Drugs for intubation • 37# 左管 • Check position by fiberscope and fixed • A-line • CVP
PSVT was noted during CVP insertion • EKG showed PSVT when guide wire was inserted • Adenosine was used for treatment via CVP • 6 mg initial iv push , but in vain • Another 12 mg iv push about 1 min later • After bradycardia was showed for seconds, EKG was returned to sinus rhythm
High pressure was alarmed by monitor!! • Rechecked tube position • High pressure was still noted • EtCO2 and BS was decreased • SpO2 was slight decreased • Call VS, and check tube again • High EtCO2 (around 70) was noted • Bronchspasm was noted at RLL
Wheezing was heard after EtCO2 was showed • Steroids and aminophylline were given immediately. • Mild wheezing was noted 10mins later. • No episode was noted during operation • No wheezing was noted at the end of surgery
Life Sciences. 69(11):1225-40, 2001 Aug 3 • Bronchospasm induced by adenosine is blocked by representatives of all the major classes of drugs used in the treatment of asthma. • Clinical studies have suggested involvement of neural pathways, mast-like cells and mediators such as histamine, serotonin and lipoxygenase products. There is a strong link between responsiveness to adenosine and eosinophilia. • In different animal models A1, A2b and A3 adenosine receptor subclasses have all been implicated in inducing bronchospasm. • At least two different mechanisms, both involving neural pathways, exist. One, involving the adenosine A1 receptor, functions in mast cell depleted animals; the other requires interaction with a population of mast-like cells activated over A2b or A3 receptors.
Life Sciences. 69(11):1225-40, 2001 Aug 3 • Not only histamine but also serotonin and lipoxygenase products released from the mast-like cells are potential mediators. • As mast cells both release adenosine and respond to adenosine, adenosine provides a non-specific method of amplifying specific signals resulting from IgE/antigen interaction. • This mechanism may not only have a pathological significance in asthma; it may be part of a normal bodily defense response that in asthmatic subjects is inappropriately activated.
Is the dyspnea during adenosine cardiac stress test caused by bronchospasm? American Heart Journal. 142(1):142-5, 2001 Jul. • Adenosine cardiac stress is widely used as an alternative to exercise testing during myocardial perfusion imaging (MPI). Dyspnea often accompanies the adenosine stress test. • Although known asthmatic patients are excluded from this test because of the danger of bronchospasm, there is incomplete information regarding the role of factors such as chronic obstructive pulmonary disease (COPD) and tobacco smoking in adenosine-induced dyspnea.
American Heart Journal. 142(1):142-5, 2001 Jul. PATIENTS AND METHODS: A total of 122 consecutive patients (75 male, 47 female; mean age 59 years, SD 10 years) undergoing pharmacologic stress testing with an intravenous infusion of adenosine also had volume-flow spirometry (Vitalograph Compact, Vitalograph Ltd) before, during, and after the test. The indices assessed were forced expiratory volume in one second, its ratio to the forced vital capacity, and peak expiratory flow rate.
American Heart Journal. 142(1):142-5, 2001 Jul. RESULTS: Mild to severe symptoms were experienced by 81% of patients during adenosine infusion. More than half the patients had dyspnea, but there was no associated bronchospasm. Although the patients with COPD showed parameters indicative of bronchial resistance compared with those without this problem, there was no further deterioration after adenosine infusion. Similarly, patients with a history of tobacco abuse, despite showing a tendency toward increasing airways resistance, had no bronchospasm during the administration of adenosine.
American Heart Journal. 142(1):142-5, 2001 Jul. CONCLUSIONS: • Although dyspnea is a common problem during adenosine stress MPI, it is not associated with any appreciable bronchospasm. • COPD and tobacco abuse do not appear to be contraindications to adenosine stress MPI studies. However, it is probably safe to exclude patients with severe COPD from adenosine stress MPI until after further evaluation with larger numbers of patients.
Pulmonary function monitoring during adenosine myocardial perfusion scintigraphy in patients with chronic obstructive pulmonary disease. CONCLUSION: This study shows that adenosine can be safely administered intravenously to selected patients with known or suspected COPD to produce coronary vasodilatation for myocardial perfusion imaging. Patients who are within the guidelines established for this study should be considered for adenosine coronary vasodilatation with use of bronchodilator pretreatment, a graduated dose of adenosine, and regular chest auscultation during the infusion. Mayo Clinic Proceedings. 74(4):339-46, 1999 Apr.
Prednisolone hastens recovery from histamine-induced bronchospasm in asthmatics. Journal of Asthma. 37(5):435-40, 2000 Aug.