Download
1 / 1
10 likes | 201 Vues
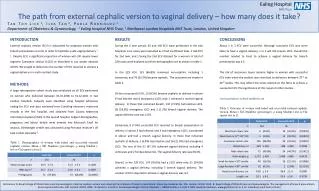
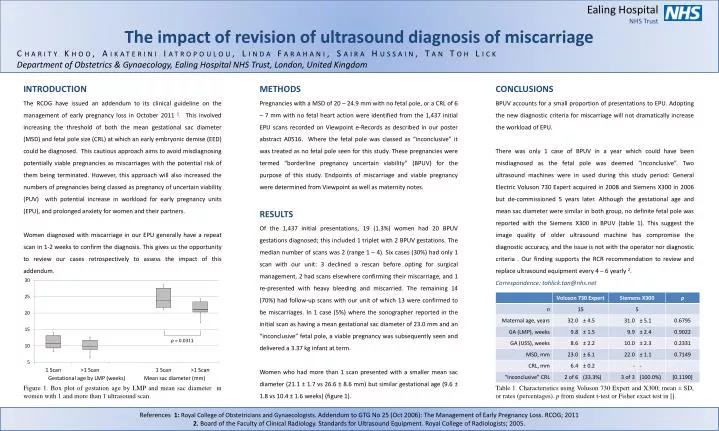
Ealing Hospital NHS Trust The impact of revision of ultrasound diagnosis of miscarriage Charity Khoo, Aikaterini Iatropoulou, Linda Farahani, Saira Hussain , Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
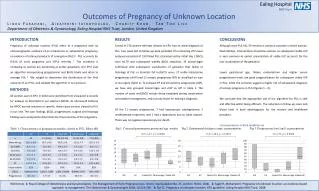
Ealing Hospital NHS Trust The impact of revision of ultrasound diagnosis of miscarriage Charity Khoo, Aikaterini Iatropoulou, Linda Farahani, Saira Hussain, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION The RCOG have issued an addendum to its clinical guideline on the management of early pregnancy loss in October 2011 1. This involved increasing the threshold of both the mean gestational sac diameter (MSD) and fetal pole size (CRL) at which an early embryonic demise (EED) could be diagnosed. This cautious approach aims to avoid misdiagnosing potentially viable pregnancies as miscarriages with the potential risk of them being terminated. However, this approach will also increased the numbers of pregnancies being classed as pregnancy of uncertain viability (PUV) with potential increase in workload for early pregnancy units (EPU), and prolonged anxiety for women and their partners. Women diagnosed with miscarriage in our EPU generally have a repeat scan in 1-2 weeks to confirm the diagnosis. This gives us the opportunity to review our cases retrospectively to assess the impact of this addendum. Figure 1. Box plot of gestation age by LMP and mean sac diameter in women with 1 and more than 1 ultrasound scan. METHODS Pregnancies with a MSD of 20 – 24.9 mm with no fetal pole, or a CRL of 6 – 7 mm with no fetal heart action were identified from the 1,437 initial EPU scans recorded on Viewpoint e-Records as described in our poster abstract A0516. Where the fetal pole was classed as “inconclusive” it was treated as no fetal pole seen for this study. These pregnancies were termed “borderline pregnancy uncertain viability” (BPUV) for the purpose of this study. Endpoints of miscarriage and viable pregnancy were determined from Viewpoint as well as maternity notes. RESULTS Of the 1,437 initial presentations, 19 (1.3%) women had 20 BPUV gestations diagnosed; this included 1 triplet with 2 BPUV gestations. The median number of scans was 2 (range 1 – 4). Six cases (30%) had only 1 scan with our unit: 3 declined a rescan before opting for surgical management, 2 had scans elsewhere confirming their miscarriage, and 1 re-presented with heavy bleeding and miscarried. The remaining 14 (70%) had follow-up scans with our unit of which 13 were confirmed to be miscarriages. In 1 case (5%) where the sonographer reported in the initial scan as having a mean gestational sac diameter of 23.0 mm and an “inconclusive” fetal pole, a viable pregnancy was subsequently seen and delivered a 3.37 kg infant at term. Women who had more than 1 scan presented with a smaller mean sac diameter (21.1 ± 1.7 vs 26.6 ± 8.6 mm) but similar gestational age (9.6 ± 1.8 vs 10.4 ± 1.6 weeks) (figure 1). CONCLUSIONS BPUV accounts for a small proportion of presentations to EPU. Adopting the new diagnostic criteria for miscarriage will not dramatically increase the workload of EPU. There was only 1 case of BPUV in a year which could have been misdiagnosed as the fetal pole was deemed “inconclusive”. Two ultrasound machines were in used during this study period: General Electric Voluson 730 Expert acquired in 2008 and Siemens X300 in 2006 but de-commissioned 5 years later. Although the gestational age and mean sac diameter were similar in both group, no definite fetal pole was reported with the Siemens X300 in BPUV (table 1). This suggest the image quality of older ultrasound machine has compromise the diagnostic accuracy, and the issue is not with the operator nor diagnostic criteria . Our finding supports the RCR recommendation to review and replace ultrasound equipment every 4 – 6 yearly 2. Correspondence: tohlick.tan@nhs.net Table 1. Characteristics using Voluson 730 Expert and X300; mean ± SD, or rates (percentages). p from student t-test or Fisher exact test in []. References 1:Royal College of Obstetricians and Gynaecologists. Addendum to GTG No 25 (Oct 2006): The Management of Early Pregnancy Loss. RCOG; 2011 2. Board of the Faculty of Clinical Radiology. Standards for Ultrasound Equipment. Royal College of Radiologists; 2005.