Download
1 / 1
20 likes | 392 Vues
Ealing Hospital NHS Trust Early pregnancy diagnosis at first presentation Charity Khoo, Aikaterini Iatropoulou, Saira Hussain, Linda Farahani , Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
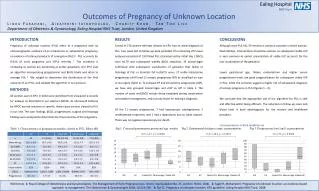
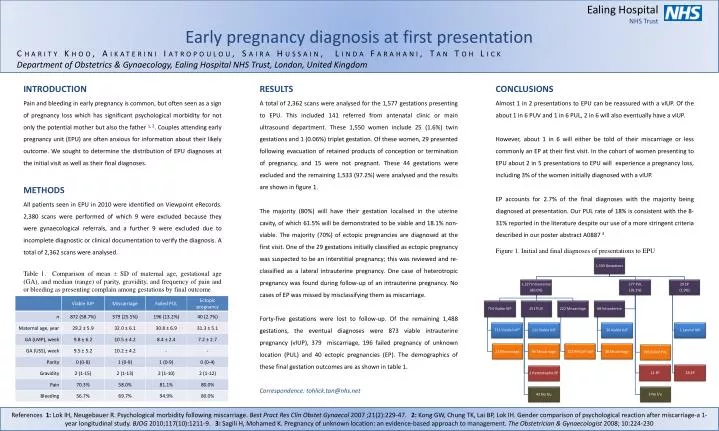
Ealing Hospital NHS Trust Early pregnancy diagnosis at first presentation Charity Khoo, Aikaterini Iatropoulou, Saira Hussain, Linda Farahani, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION Pain and bleeding in early pregnancy is common, but often seen as a sign of pregnancy loss which has significant psychological morbidity for not only the potential mother but also the father 1, 2. Couples attending early pregnancy unit (EPU) are often anxious for information about their likely outcome. We sought to determine the distribution of EPU diagnoses at the initial visit as well as their final diagnoses. METHODS All patients seen in EPU in 2010 were identified on Viewpoint eRecords. 2,380 scans were performed of which 9 were excluded because they were gynaecological referrals, and a further 9 were excluded due to incomplete diagnostic or clinical documentation to verify the diagnosis. A total of 2,362 scans were analysed. Table 1. Comparison of mean ± SD of maternal age, gestational age (GA), and median (range) of parity, gravidity, and frequency of pain and or bleeding as presenting complain among gestations by final outcome RESULTS A total of 2,362 scans were analysed for the 1,577 gestations presenting to EPU. This included 141 referred from antenatal clinic or main ultrasound department. These 1,550 women include 25 (1.6%) twin gestations and 1 (0.06%) triplet gestation. Of these women, 29 presented following evacuation of retained products of conception or termination of pregnancy, and 15 were not pregnant. These 44 gestations were excluded and the remaining 1,533 (97.2%) were analysed and the results are shown in figure 1. The majority (80%) will have their gestation localised in the uterine cavity, of which 61.5% will be demonstrated to be viable and 18.1% non-viable. The majority (70%) of ectopic pregnancies are diagnosed at the first visit. One of the 29 gestations initially classified as ectopic pregnancy was suspected to be an interstitial pregnancy; this was reviewed and re-classified as a lateral intrauterine pregnancy. One case of heterotropic pregnancy was found during follow-up of an intrauterine pregnancy. No cases of EP was missed by misclassifying them as miscarriage. Forty-five gestations were lost to follow-up. Of the remaining 1,488 gestations, the eventual diagnoses were 873 viable intrauterine pregnancy (vIUP), 379 miscarriage, 196 failed pregnancy of unknown location (PUL) and 40 ectopic pregnancies (EP). The demographics of these final gestation outcomes are as shown in table 1. Correspondence: tohlick.tan@nhs.net CONCLUSIONS Almost 1 in 2 presentations to EPU can be reassured with a vIUP. Of the about 1 in 6 PUV and 1 in 6 PUL, 2 in 6 will also eventually have a vIUP. However, about 1 in 6 will either be told of their miscarriage or less commonly an EP at their first visit. In the cohort of women presenting to EPU about 2 in 5 presentations to EPU will experience a pregnancy loss, including 3% of the women initially diagnosed with a vIUP. EP accounts for 2.7% of the final diagnoses with the majority being diagnosed at presentation. Our PUL rate of 18% is consistent with the 8-31% reported in the literature despite our use of a more stringent criteria described in our poster abstract A0887 3. Figure 1. Initial and final diagnoses of presentations to EPU References 1:Lok IH, Neugebauer R. Psychological morbidity following miscarriage. Best Pract Res ClinObstetGynaecol 2007 ;21(2):229-47. 2: Kong GW, Chung TK, Lai BP, Lok IH. Gender comparison of psychological reaction after miscarriage-a 1-year longitudinal study. BJOG 2010;117(10):1211-9. 3: Sagili H, Mohamed K. Pregnancy of unknown location: an evidence-based approach to management. The Obstetrician & Gynaecologist 2008; 10:224-230