Download
1 / 45
450 likes | 587 Vues
The Political Cost of AIDS in Africa: Examining the state of leadership, state budgets, and challenges of PLHIV in participating in political and economic life Presentations by the governance and AIDS Programme to the International AIDS Conference, Vienna, 2010.

E N D
The Political Cost of AIDS in Africa: Examining the state of leadership, state budgets, and challenges of PLHIV in participating in political and economic life Presentations by the governance and AIDS Programme to the International AIDS Conference, Vienna, 2010 Kondwani Chirambo, Director, Governance and Aids Programme, IDASA
Acknowledgements Idasa’s Governance and AIDS Programme (GAP) is sponsored by SIDA/Norwegian Team on HIV/AIDS for Africa Contributions to other Idasa studies & activities have come from: The Rockefeller Brothers Fund The Ford Foundation The Local government project sponsored by: The Netherlands Institute for International Relations The Social Science Research Council The University of Kwazulu Natal
Presentation Outline Introduction of Idasa-GAP Idasa studies on leadership Case study: Leadership Attrition in SA local government Background & problem Impact of AIDS on ward councillors in SA Impact of AIDS on political careers in SA Impact of stigma & discrimination on ward councillors in SA Conclusion; Important Questions about leadership
Democratic Governance HIV and AIDS Idasa-GAP formed in 2002 to study AIDS and Democratic governance; our interest is to ensure strong institutions, active citizenship and human dignity
Democratic AIDS Governance defined Democratic governance principles in the context of HIV & AIDS: • Visonary leadership that is able to mobilise cross sectoral support, and develop long term strategies to deal with HIV & AIDS • Broad participation from civil society in HIV policy process • association: Vibrant civil society demands delivery of good health for all • Human rights: rights of infected and affected taken into account in making AIDS policy/legislation • People are free from all forms of discrimination (HIV+ related) and have opportnities to access key elements of human development (employment, education, health) • Economic and social policies responsive to people’s needs • Free and fair elections: citizens make choices of AIDS policy & foster accountability on government performance • Freedom of assembly & Free and fair elections: citizens make choices of AIDS policy & foster accountability on government performance
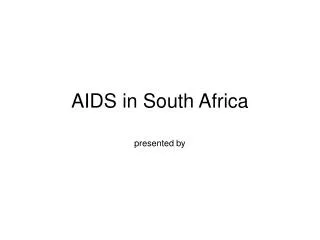
70 65 60 Botswana 55 South Africa Life expectancy at birth (years) 50 45 Swaziland 40 35 Zambia 30 Zimbabwe 25 20 1970–1975 1980–1985 1990–1995 2000–2005 1975–1980 1985–1990 1995–2000 2005–2010 Source: United Nations Population Division (2004). World Population Prospects: The 2004 Revision, database. Impact of AIDS on life expectancy in five African countries, 1970-2010
Background: Idasa-GAP studies on elected leadership in Africa • Idasa-GAP has conducted ground breaking studies in Zambia, Zimbabwe, Malawi, Tanzania, Namibia, South Africa and Senegal between 2002-2008, amongst parliamentarians • Those studies have shown that there has been high attrition amongst relatively young MPs in hyper endemic countries (particularly Malawi, Tanzania, Zambia, Zimbabwe, during the ‘aids era’ (i.e. since 1985) • This is not the case in countries with low prevalence such as Senegal, where impact was insignificant
Idasa-GAP studies on local governance and leadership in Africa • In 2009, Idasa-GAP launched studies to understand how AIDS affects political systems and finances in local government • Studies are being carried out in conjunction with partners in Southern, Eastern and Western Africa • Studies involve state and on state actors. They aim to contextualise responses to capacity of each local entity
Examining the case of South Africa AIDS, Leadership & local governance in South Africa, 2009
Background: HIV & AIDS in SA HIV AND AIDS ESTIMATES • Number of people living with HIV: 5 700 000 [4 900 000 - 6 600 000] • Adults aged 15 to 49 prevalence rate: 18.1% [15.4% - 20.9%] • Adults aged 15 and up living with HIV: 5 400 000 [4 700 000 - 6 200 000] • Women aged 15 and up living with HIV: 3 200 000 [2 800 000 - 3 700 000] • Children aged 0 to 14 living with HIV: 280 000 [230 000 - 320 000] • Deaths due to AIDS: 350 000 [270 000 - 420 000] • Orphans due to AIDS aged 0 to 17: 1 400 000 [1 100 000 - 1 800 000] (Epidemiological Fact Sheet on HIV and AIDS Core data on epidemiology and response: (South Africa, UNAIDS/WHO, 2008)
Defining Leadership: an IAS Perspective In the IAS definition, leaders material at all levels: • National governments, UN agencies, bilateral/multilateral and private donors, persons living with HIV/AIDS, Parliamentarians, • Researchers, civil society and community activists, the private sector, • Media and individual role models. Leaders are found at all levels, in all sectors and regions; they are young or old, male, female or other gender.
Why leadership is important in HIV & AIDS responses • make decisions and control resources; • have the credibility and legitimacy to lead; • have a constituency they can mobilize; • influence and/or have the potential to influence thousands or millions; and/or • inspire and have the ability to bring about change (IAS). • The Idasa GAP studies focus on elected leaders because they decide our governance priorities, including the allocation of AIDS resources
Methodology This presentation is drawn from a much larger project which used the following methods: • Statistical analysis: IEC mortality data from the electoral data base and HIV/AIDS data provided a basis for drawing inferences on the potential AIDS deaths among the elected representatives and registered voters who form part of their communities. • Interviews: interviews 112 ward councillors HIV/AIDS managers in 12 local municipalities, municipal managers, and Integrated Development Plan (IDP) managers in the four provinces • Focus group discussions: 8 FDGs with 74 community participants assisted us to understand levels of expectation in terms of service delivery from their ward councillors • Extensive literature reviews of AIDS journals, publications on State fragility, local government reports and Afrobarometer studies on local government were also undertaken.
Interviews were conducted in 12 local municipalities in four provinces
Focus of Study is on the Political System of LG; Ward Councillors nation-wide • In the South African study we focussed on the directly elected representatives who number 3 895 out of 8 951 councillors (the balance of whom are assigned through proportional representation). This was done nationally. • The means by which we track attrition among directly elected councillors is through the causes of by-elections between the year 2000-2007. • We analyse the ages of councillors. Where there is a preponderance of deaths among councillors between 22- 49 years, inferences may be drawn on the possible causes of such a mortality profile. • We compare the trends in deaths to AIDS mortality in the general population. Is there a correspondence in patterns?
The Challenge of HIV & AIDS to sustainable Leadership • While embracing the conferences’ definition, we emphasise that in the age of AIDS successful leadership should be characterised by sustainable rate of replacement. • And precisely because of AIDS we are tempted to ask the question: • how effective is leadership when it is faced with the same rate of attrition as the general population • What are the implications of having a leadership that is itself infected by HIV?
Key points of inquiry on leadership • Knowledge and experience of HIV & AIDS • Disclosure and its implications on political careers • Policies and proposals for dealing with HIV & AIDS in local government institutions and communities • Lastly, we made some conclusions about the implications of rapid attrition of leadership for institutional capacity
The problem: Potential for weak local government • Capacity issues in local government: even without AIDS, the ambitions of local government in South Africa since 1993 appeared compromised by a myriad capacity-related issues; capacity, shortage of skills, leading to poor service delivery • Provision of health, water & sanitation, spatial land management & social services is still at the centre of controversy
Public perception of local government performance (2004-2006) Afrobarometer (2006)
Public perception of local government performance (2004-2006) • Afrobarometer Studies of 2006 shows that all South Africans judge local government performance in terms of their perceptions of whether the elected councillor is doing a good job. • The levels of satisfaction are lower among rural folk than urban populations. Black people are the least satisfied of the races. • While conceding that the period 2004–2006 was too short to anticipate any significant trends, the study shows that the number of South Africans who believe the government is handling affairs well at local level is in decline. • The four provinces without metropolitan councils – Mpumalanga, Limpopo, North West and Northern Cape –reported the highest dissatisfaction.
Public perception of local government performance (2004-2006) • Notwithstanding the prospect that the roles and responsibilities of councillors may be ill-understood by their constituencies, the blame seems to lie squarely at the elected officials’ doorstep. • We infer these developments and from Afrobarometer public opinion surveys that councillors are seen as agents of change/development as well as local legislators. • The adult population of South Africa would hence expect their material well being to be advanced by the councillors whom they elect every five years through the MMP system.
AIDS can complicate negative perceptions of local government and leaders • Firstly, we glean from this that it would be problematic if councillors absent themselves from community engagements or are ineffective due to HIV/AIDS related illnesses • The same logic might apply if there is a death of a highly competent councillor due to AIDS or any other illness or cause: • The loss of representation might be especially problematic in communities with restive populations, who are already unhappy with service delivery • Secondly, stigma and discrimination can be a barrier to political participation: could we therefore expect councillors who are known to be HIV positive confidently performing their duties despite these barriers? • We began this study by examining the trends in mortality amongst ward councillors to infer the possible influence of AIDS
FINDINGS: Mortality amongst ward councillors • IEC records show that nationally, a total of 589 • By-elections were held between 2001-2007 • Death was the leading cause of by-elections (or vacancies) at 48,7% (285 by elections held as a result) • Compared to resignation at 40,9%, termination of councillor membership by party at 7,5%, dissolution of council by MEC 2%, expulsions 0,8%, and imprisonment 0,1%.
Findings: Mortality Amongst Ward Councillors Nationally (2001-2007)
Councillor deaths by Gender 2001-2007 • The highest number of deaths (absolute) among men was recorded in 2004 and 2005. • The data shows that male deaths totalled 217. • The highest female mortality figures were recorded in 2003 and 2007. Deaths fluctuated over the years but peaked in 2003 for females. • On average, 31 male councillors died per year for the seven years, compared to eight female councillors for the same period • There are probably more males councillors than females in LG (numbers not ascertained)
Deceased Female and Male Councillors • The gender-disaggregated data shows that: • deaths among female councillors are concentrated in the 40–44 and 45–49 age groups • In 2001, male councillors in the 35–39 and 25–29 age groups accounted for 21% of all the deaths among this gender; • While the 60–64 age cohort accounted for only 3,4%. • The largest number of councillors to die came from the 45–49 age group and accounted for 23% of deaths.
Life expectancy & ART • Dorrington et al. (2006) assert that AIDS has subtracted 13 years off the life expectancy of South Africans, reducing it from 64 years to 51 years. • The mortality profile described by WHO (2006) and Dorrington, et al. (2006) certainly reflect similarities in the trends in deaths observed among ward councillors in South Africa. • In the age of treatment, it is suggested that South Africans will live longer. • Dorrington, et al. (2004) also indicate that 70% of all deaths in 2004 in the 15–49 age group were due to AIDS. The figure declined to 45% when all adults (15+) were factored in.
Life expectancy & ART • If these statistics were taken as a constant over the 2001–2007 period, we could assume that 70% of the councillors passing away in South Africa over this period died of AIDS. However, this would require us to make further assumptions: • Councillors are universally representative of all South Africans. • Gender of the councillors is of a representative parity. • A constant AIDS death ratio applies to all of South Africa for the period 2001–2007. • An even distribution of HIV/AIDS prevails across the entire country. • Based on this reasoning, Figure 9 shows that 70% of mortality among councillors in the 22–49 age group is attributable to AIDS
Councilor deaths with 70% AIDS ratio factored in (22-49 year olds)=163
Impact of stigma & discrimination on ward councillors: Disclosure (interviews: N=112) Disclosure: fear of ostracism that influences attitudes towards disclosure, VCT & ART. • Political leaders fear rejection, but anyone can get it. • (Councillor, Piketberg) • It is kept a secret, so we do not really know who has died from AIDS (Councillor, Steinkopf) • Some of the people will think that everyone one in the party is sick, (councillor, Ladybrand) • I was the first one to give the example by taking the test. • (Councillor, Kimberley)
Impact of stigma & discrimination on ward councillors: disclosure • To our knowledge, there is only one councillor living with HIV/AIDS in South Africa (openly) • The councillor is the only known elected representative living with HIV/AIDS in Sub Saharan Africa • Studies on parliament by Idasa show high attrition amongst MPs in the SADC region but no disclosure • Despite presence of policies, knowledge is poor and ART uptake reportedly weak due to fear of exposure
Community Activists demand openness on HIV / AIDS from councillors (8 FDGs. N=74) • Community expectations of councillors are high, though they are disappointed with outcomes • Service delivery: Favourable achievements were attributed to central government, there was little reference to councillors as drivers of hope and change in relation to HIV/AIDS. • Openness of leadership about HIV status demanded • Majority had no problems voting for an HIV-positive councillor
Implications: Deaths and illness will weaken effectiveness and accountability in political system Implications; weak governance - compromises confidence and may contribute to discontent among communities • Institutional memory: Lesser experienced leadership emerging from HIV and AIDS due to attrition among experienced leaders may not perform to the same levels of effectiveness • Leadership withdrawal due to illness: A fear of rejection by the electorate may lead to lack of effectiveness and accountability • Ineffectiveness and lack of accountability might fuel discontent amongst restive communities
Implications: Deaths and illness may lead to lack of legitimacy • Legitimacy: By elections exhibit poor turn outs which may create crises in legitimacy which results in weak mandates (Turn out average 38%) • AIDS may cause weak administrative systems due to attrition amongst professional and general workers, therefore the support systems to the political system are themselves affected. • So far only anecdotal evidence exists. Local municipalities in this study indicate that absenteeism and deaths amongst staff are emerging issues.
Implications: The governance dynamic Impact of councillor attrition on political parties • Leadership: compromise the ability of small parties to regain their seats through by-elections • Finance: Larger parties would be better financed through the party financing system • Administration / electioneering: Death of a leader/s impact on parties’ organisational structures, weakening ability to compete effectively
Implications: The governance dynamic Political costs of by-elections: Power shifts in SA (2001-2007)
Implications: Economic costs of replacing councillors through First-Past-the-Post system (SA uses Mixed system) • Cost of by-elections & sustainability: According to the IEC of South Africa, a ward by-election costs, on average, R25 000 (US$3 333) (Interview: Hendrickse). • Based on this figure, South Africa spent at least R14,7 million (US$1,9 million) on hosting by-elections between 2001 and 2007. • At least half of that amount – R7,1 million (US$946 667) was spent in the wards where councillors died of undisclosed causes, • Compared to R6 million (US$800 000) to fill vacancies caused by resignations,
Conclusions • Despite a mortality profile that is not dissimilar to the AIDS mortality profile in the general population, there is only one elected leader in the whole of Africa (to our knowledge), who lives with HIV. • This will have implications for community confidence in their elected leaders as signified by the focus group participants who demand openness as an integral part of leadership • There is clearly a problem of leadership maintenance in local government in South Africa compounded by an unusually high mortality rate amongst politicians below the age of 51. This compromises institutional memory and continuity and could harm the relation between governor and governed • We believe the consequences of AIDS on leadership need to be diagnosed early, given the broad implications for service delivery
Conclusions There is a whole range of capacity matters that can be recommended. In our view however, there is need to have a degree of citizen involvement in developing a responsive elected leadership at local and national levels • Idasa-GAP is testing a diagnostic tool which would assist identify problems associated with HIV & AIDS within local government, that would contribute to institutionalisation and wider ownership of the epidemic and its responses • The tool will hopefully also assist with addressing the issue of capacitating in-coming leadership and maintaining them over time in local government---this tool shall be presented by Ms Phoebie Machere