Download
1 / 44
480 likes | 841 Vues
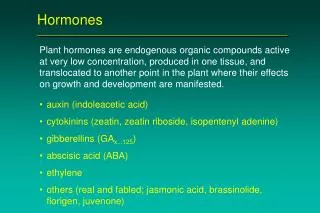
Sex hormones . . Regulators. gonadotropin-releasing hormone (GnRH ) follicle-stimulating hormone (FSH) luteinizing hormone (LH). Intensity of hormonal secretion in the cycle. Feed back-regulation. Biosynthesis of steroids. Estrogen-functions. IN WOMEN

E N D
Regulators • gonadotropin-releasing hormone (GnRH) • follicle-stimulating hormone (FSH) • luteinizing hormone (LH)
Estrogen-functions IN WOMEN Developmental effects, neuroendocrine actions- in the control of ovulation- Cyclical preparation for fertilization ACTIONS Mineral,carbohydrate,protein and lipid metabolism Estrogens and males on bone, spermatogenisis,& behaviour
Benefits associated with postmenopausal estrogen replacement .
SiDE Effects ---Estrogens Nausea vomiting Breast tenderness Migraine headache Uterine bleeding Hyper pigmentation Cholestiasis Gall bladder disease Edema Hypertension Breast cancer
Hormonal contraceptives ORAL, PARENTERAL & IMPLANTED CONTRACEPTIVES O.C – 1.Combinations of estrogens and progestins 2.Sole progestin therapy FORMS Biphasic Triphasic Monophasic Dosage of one or both components changed twice during the cycle Dosage of one or both components changed Once during the cycle No change of both components during the cycle
Estrogens and progestins -clinical use • Contraception • Hormone replacement therapy-post menopasal, hypogonadism, (along with Gonadotropins/growth hormones in delay) • Antiprogestins abortifacients, contraception • Estrogen antagonists estrogen dependent neoplasm
Transport - Kinetics Estradiol binds to α2 globulin (SHGB) And to albumin in lower affinity. Estradiol Liver estrone, estriol 2hydroxylated derivatives Conjugated metabolites Water soluble excreted in bile Small amounts in breast milk Can be activated in the intestines Hepatic first pass effect is minimized by other routes-Transdermal, Vaginal or by injection.
Mechanism of action Steroid hormones diffuse across the cell membrane and bind with high affinity to specific nuclear receptor proteins Ligand – receptor complex Forms a dimer before binding DNA PRE -ORE Activate gene transcription hormone-specific RNA synthesis synthesis of specific proteins that mediate a number of physiologic functions
Mechanism, Effects of contraceptives Combinational Contraceptives block pituitary function Leads to inhibition of ovulation Continuous use of progestin alone does not always inhibit ovulation Combinational agents also produce change in the cervical mucus in the uterine tubes all of which decrease The likelihood of conception and implantation Effects on ovary- depress ovarian function Effects on uterus- Hypertrophy and polyp formation Effects on breasts- Enlargement, suppress lactation, less amt. transverse in to milk CNS--------------- estrogen excites, progestin depress the brain Endocrine –inhibition of gonadotropins, adrenal structure d function, high conc. Increase in α2 globulin Blood- increased coagulability, increased dosage of coumarin analogs required, increased sr. iron and total iorn binding capacity.
The figure below shows the mechanism of action of Viagra, and the other PDE5 inhibitors, on the nitric oxide cycle.
Erectile dysfunction = consistent inability to obtain and/or maintain an erection sufficient for satisfactory sexual relationsNIH 1992
Risk factors for ED • Vasculogenic factors • Age • Certain medications • Psychosocial/psychological factors • Neurogenic factors • Hormonal factors
Endothelial dysfunction is a risk factor for CVD and ED Heart failure Atherosclerosis Smoking Hypertension Oxidative stress Diabetes Endothelial dysfunction ED Adapted from Rubanyi GM. J Cardiovasc Pharmacol 1993; 22 (Suppl 4): S1–S4
Causes of ED • Organic(80 %) • diabetes mellitus, hypertension, hyperlipidemie, benign prostate disease, peripheral vascular disease, cardiac problems, hormonal problems (pituitary, testis, thyroid, adrenal), neurogenic (cerebral, spinal, dorsal nerve, cavernous nerve) • postsurgical: radical prostatectomy, abdominoperineal resection • Psychogenic, drugs (20 %)
Alcohol Estrogens Antiandrogens H2 receptor blockers Anticholinergics Ketoconazole Antidepressants Marijuana Antihypertensives Narcotics ß-blockers Psychotropics Cigarettes Cocaine Spironolactone Lipid-lowering agents NSAIDs Cytotoxic drugs Diuretics Drugs Associated with ED
Causes of ED • Neurogenic • Parkinson´s disease – 60% • Multiple sclerosis – 70% • Spinal cord trauma, tumor etc. • Peipheral neuropathy: diabetes, alcoholism, chronic renal failure
Diagnosis of ED may uncover other serious treatable disorders • Hypertension • 68% of men with hypertension had ED to some degree • Dyslipidemia • 60% of men with ED had dyslipidaemia • Heart disease • 56% of men with ED were found to have a positive stress test • 40% of men with ED had significant coronary occlusions
Oral therapy • PDE 5 inhibitors (95%) • 2-blockers (Yohimbin) • hormonal therapy (testosterone)
Phosphodiesterases • Main role: termination of cyclic nucleotide second messenger signal, often cGMP • 11 PDE groups (PDE 1-11) • PDE-5 breaks down cGMP (the second messenger of Nitric Oxide—NO), reversing the muscle-relaxant effect of NO • PDE-5 is found in corpus cavernosum, vascular and visceral muscles, and in platelets
N.O. Release Increases Penile Bloodflow Lue,T. NEJM 2000. 342:1802
O O O O H N H N O N N O H N H N N N N N N N N N N H N 2 O O 0H O S O O S O O O N O O N P O 0 H N Tadalafil cGMP N Sildenafil Vardenafil O CH3 H3C O CH3 Caffeine PDE5 inhibitors
PDE5: localization • PDE5 is localized in vascular smooth muscle cells • PDE5 is not localized in the following: • cardiac myocytes • endothelial cells • lymphatic cells • cardiac conduction tissue
PDE5 inhibition with sildenafil Sexual stimulation Corpus cavernosum Erection NANC NO Smooth muscle relaxation of the cavernosal arteries & the corpora cGMP GTP GMP PDE5 NO=nitric oxide; NANC=nonadrenergic-noncholinergic neurons; PDE5=phosphodiesterase type 5
PDE5 Inhibitors: Pharmacokinetics 1Klotz et al. ACCP. 2002;2 As reported in Kim et al. Formulary. 2002;37. *Median (range).
PDE5 inhibitors – side effects sildenafil tadalafil vardenafil (N = 724/379)(N = 1812/793) headache15%14,5 / 5,5% - placebo 16 / 6% dyspepsia6%12,3 / 1,8% 4 / 1% backache 0%6,5 / 4,2% 0% rhinitis 2%4,3 / 3,2% 10 / 4% myalgia0%5,7 / 1,8% 0% flushing 14%4,1 / 1,6% 12 / 1% abnormal vision 5%0%<2 / 0%
Contraindications • Since PDE5 inhibitors such as sildenafil, tadalafil, and Vardenafil may cause transiently low blood pressure (hypotension), organic nitrates should not be taken for at least 48 hours after taking the last dose of tadalafil. Using organic nitrates within this timeframe may increase the risk of life-threatening hypotension.