Download

1 / 27
280 likes | 468 Vues
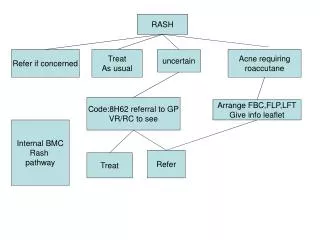
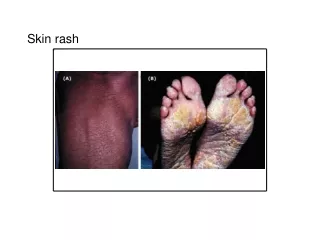
Infections with Rash. By Prof. Samir Zamzam Ped. Department Zagazig University. Rash may be macule, papule, vesicle, pustule, crust. and hemorrhagic rash. Meningitis Means inflammation the brain meninges Dura, Archanoid and pia from outside to inside. Causative organisms:

E N D
Infections with Rash By Prof. Samir Zamzam Ped. Department Zagazig University
Rash may be macule, papule, vesicle, pustule, crust. and hemorrhagic rash. Meningitis Means inflammation the brain meninges Dura, Archanoid and pia from outside to inside. Causative organisms: Neonatal periode and early infancy: • Group B streptococci • Gram –ve enteric bacilli (E. coli) • Lepospirosis • H. influana type B Later infancy and childhood: • H. influenza type B. • Pneumococci • Meningiococci • Staphilococci • Rarely any other organisms.
Meningiococcal Meningitis Gram –ve cocci (Neisseria meningitides) A commensal in the nasophynx of healthy individual. • Meningiacoccemia occur when the organism invade the blood stream and disseminate to various parts of the body.
Pathogenesis: The cell wall of the organism contains a lipo-polysaccharide (endotoxin) responsible for serious systemic manifestations. This endotoxin leads to systemic toxemia, prepheral circulatory failure, DIC, bleeding in the adrenals leads to shock (waterhouse-Fredrichsen-syndrome). Mode of infection droplet infection as the primary focus of infection is in the nasopharynx.
Clinical features: Incubation periode 2-10 days. Upper resp. tract infection with or without bacteremia a self limited common cold like illness. Acute meningio-coccemia manifest by fever, malaise, headache and GIT upset. Followed by rash peticheal or purpuric (The hallmark of the disease). Hypotension, oliguria with progressive renal failure and coma. Meningiococcal meningitis due to haematogenous spread to meninges progressive drowsiness, vomiting, neck stiffness and convulsions, Kerng's and prudazinski signs +ve.
Diagnosis: Clinical manifestions. Culture from the nasopharynx Isolation of the meningiocicco. Blood culture. L.P and CSF examination, cells, protein, glucose, CSF culture. Site of L.P space between (L3-L4 and L4-L5). Must be done in left lateral position. Contraindication of L.P: Skin infection at the site, Bleeding tendency verteberal column deformities.
Treatment: The drug of choice is penicillin 250,000 unite 1kg/day in 6 devided doses. Ampicillin 300 mg/kg/day. Cefotoxime 200 mg/kg/day. Chloramphenical 100 mg/kg/day. Prevention vaccination for children after 2 years of age immune response lasts for about 2 years.
Chrokenpox (Varicella) A highly communicable disease. Infection is through direct or indirect contact. It is a self limited infection in children except in immunompromised children may be fatal. The causative agent DNA virus of the herpes groups (Varicella zoster virus) may remain latent to cause herpes zoster in later life.
Clinical futures: Incubation periode 15 days. Prodromal stage malaise, low grade fever, headache. Sometimes the onset may be sudden with the appearance of rash. the first sign in majority of cases. The rash pass through all stages macule, papule, vesicles, pustule crust. all stages are present in the sametime pleomorphic centripetal rash moving towards the center. Itching is mild at first but may become severe in the pustular stage. Hemorrhagic, neonatal chicken pox may occur when the mother develops chickenpox 5 days before and 5 days after delivery.
Diagnosis: Clinical manifestations. CBC WBCs may be normal, low or increased. Treatment: Symptomatic treatment. A cyclovir effective when given early. Avoid aspirin as antipyretic to prevent development of Reye's syndrome. Itching treated by antihistamines oral or local applications Calamine, potassium paramanganate.
Complications: Skin infection, purpura fulminans due to DIC, ITP. Bronchopneumonia, Encephalitis myocarditis, hepatitis, appendicitis. Prevention: Vaccination
Measles (Rubeola) The most common and the most infectious of viral infection of childhood. Characterised by catarrhal symptoms followed by a typical rash the so called measly rash. Meales is unusual before 3 to 4 months of age and mild in the next 6 months Because of protection by the maternal antibodies. One attack confers nearly life long immunity. Transmission by direct or indirect contact and droplet infection.
Clinical manifestations: Prodromal stage 3-5 days characterized by upper respiratory tract infection, conjunctivitis – cervical lymphadenopathy, fever – Koplik;s spots on the buccal mucosa. Eruptive phase 3 to 5 days after the onset with the appearance of rash fever tends to regress. Face and areas behind ears are the sites of the first appearance of rash the rash disappear in the order of appearance. Its lasts for 4-7 days. Convalescent phase is marked by disappearance of fever and other constitutial symptoms and rash. Browny pigmentation and pealing of the skin appear.
Diagnosis: Roseola infnatum (fifth disease) Rubella (Jerman measles) Infectious mononucleosis (glandular fever). Meningiococcemia. Treatment: Symptomatic Complications: Otitis media, chest infection (Bronchopneumonia), Keratitis, Activation of T.B, Malnutrition, encephalitis. Prevention vaccination at 9 months of age Revacination at 15 months
German measles (Rubella) - Mild infection - Incubation periode 2 to 3 weeks. - Propdramal stage lasts for few day (one to 2 days). Rash may be the first visible sign. It is a macule which spreads from the face to trunk. The rash disappears by the third day. Congenital Rubella syndrome
German measles (Rubella) Transmission of infection from the mother to the fetous especially during the frist the trimester. Its important manifestations are growth retardation, mental retardation, Hepatosplenmegaly, hepatitis, deafness, otitis media, pancreatitis, cleft palate, spinatifida, microphtholmia cataracts, retinal lesions. Prevention – vaccination MMR at 15 months revaccination at 10-12 years in females.
Other Pediatric Infections Mumps (Epidemic Parotitis) Infectious viral disease charact by painful swelling of salivary glands especially parotids. Clinical manifestations: Prodnormal stage: Is short 1-2 days fever, malaise, sore throot, carachic and pain behind the ear on showing and swallowing. Tender opedemaious swelling of the parotid (unilateral or bilateral). Tenderness disappear 1-3 days. Swelling disappear after 7-10 days. Infection leave life long immunity.
D.Diagnosis Suppurative parotitis. Recurrent parotitis secondary to allergy or calculus in the stensen;s duct. Paroatitis from HIV, carsacke A, cytomegalovirus. Diagnosis: - Clinical, picture. - C.B.C leucopenia and lymphocytosis. - Treatment of Symptomatic - Prevention vaccination MMR Complications: Orchitis, epididmitis Pancreatitis Meningeoencephalitis Myocarditis, nephritis, hepatitis arthritis, deafness.
Poliomeylitis Acute viral infection characterized by clinical manifestations varing from nil to rapid paralysis and even death. The disease occurs exclusively in humans. Worldwide prevalence. The majority of paralytic cases occurs below the age of 3 years. Clinical manifestations. The incubation periode 7-14 days. The clinical presentations are: Asymptomatic (silent) Abortive viraemia but Not involving CNS
Poliomeylitis Non paralytic encephalic presentation Paralytic - Spinal - Bulbar - Bulbospinal - Encephalitic Paralysis usually involve large muscles and asymmetrical. Most deaths in poliomyelitis is form respiratory failure due to involvement of the vital centers.
D. Diagnosis: Guillian burre syndrome. Transverse myeloitis CNS infections (meningitis, encephalitis). Botulism. Septic arthritis. Sever hypokalamia.
Treatment: Hospitalization. Strect bed rest. Minimal handing of the affected parts. Analgesics and mild sedation. Physiotherapy, Prevention: Vaccinations (Sabin) OPV live attenuated vaccine (Salk) Parenteral poliovaccine killed vaccine pulse immunization in order to eradicate poliovirus.
Petrussis (Whooping cough) Pertussis is a highly communicable bacterial infection. Causative organism is a nonmotile, rod-shaped gram-negative bacillus (Bordetella pertussis). Transmission by droplet infection and occasionally by contact with contaminated objects. Incubation periode one to 3 weeks.
Clinical manifestations: Catarrhal stage onset insidious Rhibitis, sneezing, lacriomotion, irritating cough which nocturnal. Paroxysmal (Spasmodic stage): Cough comes in paroxysms and is accompanied by vomiting. Series of cough in expiration followed by a sudden deep violent inspiration with characteristic sound whoop. due to laryngeospasm. Patient appear suffocated with congested (Red face). Paroxysm may be triggered by eating yowing, sneezing, drinking and any other sudden movement. Convalescent stage: disturbing cough and vomiting stop.
Diagnosis: Clinical manifestations. WBCs initially low the increase to 20.000 to 50.000 with abslute lymphocytosis as high as 90%. ESR is low. Triade of whoop, lymphocytosis and low ESR is diagnostic treatment general measures, erythromycin 50 mg/kg/day 2 weeks, prevention DPT vaccination.