Download
1 / 59
600 likes | 1.01k Vues
Rash illness. PROF.DR.YILDIZ CAMCIOĞLU. Importance. A very important sign of the disease Avoid persons to be infected, İmportant for public health exa: meningoccoccemia Differential diagnosis is done by history of rash, clinical findings, laboratory results,. Definition.

E N D
Rash illness PROF.DR.YILDIZ CAMCIOĞLU
Importance • A very important sign of the disease • Avoid persons to be infected, • İmportant for public health exa: meningoccoccemia • Differential diagnosis is done by history of rash, clinical findings, laboratory results,
Definition EXANTHEM is rash on skin Lesions at mucosa are called ENAMTHEM MACULE: Red lesion due to capillary dilatation, if you press on by a glass it fades
Papule PAPULE: Red and palpable nodular lesion due to capillary dilatation, elevated from skin generally it fades if you press on it by a glass
Vesicle is a small blister containing clear fluid, may be scattered irregularly over skin or grouped in cluster • Pustule is a small elevation of skin containing pus
ERYTHEMA Localized or diffuse erythema of skin Scarlatina or erithema marginatum
PURPURIC RASHES Petechia: a small haemorrhage beneath the epidermis Ecchymoses is a larger area of haemorrhage
Erythema Nodosum • Painful, tender, firm, raised round, or oval subcutaneous nodules • At first brigth red, then change to o bluise purple • Occur over the thights and tibia
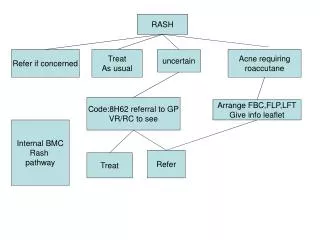
Approach to a child with rash 1- History of lesion *Date of the appearance. * Place of first appeared *Distrubution, appearance and fading * sense of pain, burning, parahestesia, pururitus 2- Experienced rash illness 3- Vaccination 4- Family history: eczema, astma, allergic rhinitis 5- Breast feeding
6- Rash illness at family, siblings, neigbourhood and school 7- Rash stimulated by:Uv, heat, food, drug, infection. 8- Other findings *Fever *Tonsillitis *Arthralgy *Growth retardation *Adenomegaly *Hepatosplenomegaly *Ichterus
EXANTEM SUBITUM, 6th Disease(ROSEOLA INFANTUM) ET: Human herpesvirus-6) EPİ: Common in fall Incubation period: 7-17 days most frequent between 6-18 months CLİNİCAL FİNDİNGS:undifferentiated febrile illness without rash or localizing signs, Fever characteristically is high (temperature greater than 39.5°C [103.0°F]) and persists for 3 to 7 days. Maculopapular rash lasting hours to days is noted once fever resolves Febrile seizures occur during the febrile period in approximately 10% to 15% of primary infections A bulging anterior fontanelle occurs occasionally
EXANTEM SUBITUM (ROSEOLA INFANTUM) , 6th disease Differential diagnosis Clinical findings Laboratory: Leucocytosis and granulocytosis on first 24-36 hours than leucopenia develops on the second day of illness No specific test for diagnosis No drug to treart
Fifth Disease;Erythema infectiosum A viral infection caused by parvovirus B19Parvovirus B19 commonly infects humans About 50% of all adults have been infected during childhood or adolescence Infected people have the virus in their saliva and mucus You can get it when you come into contact with those fluids Most people become immune to the virus after having it once
5th Disease(ERYTHEMA INFECTIOSUM) EPİDEMİOLOGY Epidemic at spring Common in school children Incubation period : 4-14 days Leads haemolytic crisis in patients with Chronic haemolitic anemia, sickle cell, spherocytosis Decreases reticulocyt count in healthy children
Symptoms Low fever, cold symptoms The ill child typically has a "slapped-cheek" rash on the face A lacy red rash on the trunk and limbs Occasionally, the rash may itch. The child is usually not very ill, and the rash resolves in 7 to 10 days. Once a child recovers from parvovirus infection, he or she develops lasting immunity,
Adults who get it might also have joint pain and swelling. Joint pain and swelling in adults usually resolve without long-term disability Fifth disease can be serious in; Pregnant women In less than 5% of all pregnant womenparvovirus B19 infection may cause a baby bornwith severe anemia or miscarriage. There is no evidence that parvovirus B19 infection causes birth defects or mental retardation Anemic children Have cancer or a weak immune system
A blood test for parvovirus B19 may show: 1) that you are immune to parvovirus B19 and have no sign of recent infection IgG(+) 2) That you are not immune and have not yet been infected IgGandIgM(-) 3) that you have had a recent infection IgM(+)
RUBELLA Etiology: Togaviridae family Rubivirus Genus RNA virus EPİDEMİOLOGY: Host is only humans, droplet infection Incubation period: 14-21 days. Prodromal stage: Mild cataral symptoms. Retroauricular, posterior cervical, occipital LAP
The cause of rubella A virus that's passed from person to person. It can spread when an infected person coughs or sneezes, or it can spread by direct contact Transmitted from a pregnant woman to her unborn child. A person with rubella is contagious from one week before the onset of the rash until about one to two weeks after the rash disappears The disease is still common in many parts of the world, although more than half of all countries now use a rubella vaccine The prevalence of rubella in some other countries is something to consider before going abroad, especially if you're pregnant
Signs and symptoms of rubella So mild that they're difficult to notice, especially in children. If signs and symptoms do occur, they typically last about two to three days and may include: Mild fever of 102 F or lower Headache Stuffy or runny nose Inflamed, red eyes Enlarged, tender lymph nodes at the base of the skull, the back of the neck and behind the ears A fine, pink rash that begins on the face and quickly spreads to the trunk and then the arms and legs, before disappearing in the same sequence Aching joints, especially in young women
Tests and diagnosis The rubella rash can look like many other viral rashes. Discrete Last 3 days Without any mark A virus culture IgG or IgM antibodies in blood
Rubella Diagnosis: 4 time increase IgG antibody or IgM(+) Vaccine: MMR 15-18 months and , 6-12 years of age Differential Diagnosis : Scarlet fever, Measles, 6th disease, enteroviral inf, infectious mononucleus, drug eruption .
Treatment Usually no need Isolation from others — especially pregnant women — during the infectious period. If a pregnant woman contract to a child with rubella ; hyperimmune globulin can be recommended This can reduce symptoms but doesn't eliminate the possibility of baby developing congenital rubella syndrome
Complications In rare cases, rubella can cause: Artritis ( on 2nd -3rd days) Encephalitis: 1/6000 Purpura: Thrombocytopenicornonthrombocytopenic Congenitalrubella
1941 reported by Gregg 1964 Epidemic in USA Up to 85 percent of infants born to mothers who had rubella during the first 11 weeks of pregnancy develop congenital rubella syndrome This can cause one or more problems, including growth retardation, cataracts, deafness, congenital heart defects and defects in other organs The highest risk to the fetus is during the first trimester, but exposure later in pregnancy also is dangerous . Congenital Rubella
MEASLES ETIOLOGY : RNA paramixovirus. EPİDEMİOLOGY : 5-10 years of age most frequent PATHOLOGY : Prodromal stage ; Hyperplasia of lymphoid tissue Coplic spots; intercellular and intracellular edema, parakeratosis, dsykeratosis Lungs: Peribronchial inflammation, interstisial mononuclear cell infiltration Cerebrum and M.spinalis: Edema, congestion and peteshial haemorage Incubation period: 8-12 days.
Transmission of Measles Spread by contact with an infected person, through coughing and sneezing (highly contagious) The disease can be transmitted from 4 days prior to the onset of the rash to 4 days after the onset. If one person has it, 90% of their susceptible close contacts will also become infected with the measles virus. The virus resides in the mucus in the nose and throat of the infected person. When that person sneezes or coughs, droplets spray into the air. The virus remains active and contagious on infected surfaces for up to 2 hours.
Pathological stages of Measles 0 day : The virus attachs epithelium of nose and throat of the infected person. Virus begin to replicate within epithelium 1-2 day: Virus spreads to local lymph nodes 2-3: Primary viremia. 3-5: Virus begin to replicate at bronchial epithelium, RES and distance areas 5-7: Secondary viremia. 7-11: Clinical findings on skin and infected areas 11-14: Virus can be isolated from blood, respiratory system, skin and other tissues 14-17: Viremia disappaers, amount of virus at tissues decreases
CLİNİCAL findings Prodromal period Symptoms high fever, cough, runny nose, and red, watery eyes (lasts about a week), Coplic spots, stimson lines Rash stage: Erythematous maculopapular are confluent Rash begins from hair-neck line, behind the ears 3rd day lesions distrubute over the foot 3-4 days later brownish spots observed instead of rash Fine desquamation also noticed Malaise can accompain to fever (+), Generalised lymphoadenopathy may be observed. Diarrhea may be seen in infancy :24-36 hours later fever decreases and symptoms disappear
Complications Approximately 20% of reported measles cases experience one or more complications common under 5 years of age ear infections in nearly 1/10 children 1/20 children gets pneumonia, 1/1,000 will develop encephalitis. 1-2/1,000 children will die pregnant woman have a miscarriage, give birth prematurely, or have a low-birth-weight baby. In developing countries, where malnutrition and vitamin A deficiency are prevalent, measles has been known to kill as many as 1/4 four people. It is the leading cause of blindness among African children. Measles kills almost 1 million children in the world each year.
MEASLES COMPLİCATIONS: Otitis, interstisial pneumonia, Secondary bacterial infections, Anergy to TB 1-2/1000 encephalomyelitis Myocarditis and mesenteric adenitis. TREATMENT: Symptomatic. A vitamine; 6 m-1 years A vit. 100 000 iU 1-2 y A vit. 200 000 iU Clinical types; Tipical Modified: who received IG (0.2 ml/kg) Atipical : who had been vaccinated Immunodeficiencies; Giant cell pneumonia
Measles vaccine (MMR, MR and measles vaccines). The MMR vaccine is a live, attenuated (weakened), combination vaccine that protects against the measles, mumps, and rubella viruses Children should get 2 doses of MMR vaccine: The first dose at 12-15 months of age The second dose at 4-6 years of age A second dose of the vaccine is recommended to protect those 5% who did not develop immunity in the first dose and to give "booster" effect to those who did develop an immune response.
Group A Beta-hemolytic streptococGAS Gram + coccus Beta-hemolytic, Alfa-hemolytic, Gamma-hemolytic Beta-hemolytics are Bacitracine sensitive Due to C=CARBONHYDRATE layer ; LANCEFİELD clasification . A-H ve K-T Due to M proteins, 75 types
Scarlet fever or Scarlatina An exotoxin-mediated disease arising from group A beta-hemolytic streptococcal infection. Ordinarily, scarlet fever evolves from a tonsillar/pharyngeal focus, although the rash develops in fewer than 10% of cases of "strep throat." Exotoxin-mediated streptococcal infections range from localized skin disorders to the systemic rash of scarlet fever to the uncommon but highly lethal streptococcal toxic shock syndrome
Frequency In the past century, the number of cases of scarlet fever has remained high, with marked decrease in case-mortality rates secondary to widespread use of antibiotics. Transmission usually occurs via airborne respiratory particles that can be spread from infected patients and asymptomatic carriers. You can get scarlet fever through direct contact with throat mucus, nasal discharge, or saliva of an infected person. The infection rate increases in overcrowded situations (schools, institutional settings).
Epidemiology The organism is able to survive extremes of temperature and humidity, which allows spread by fomites. Geographic distribution of skin infections tends to favor warmer or tropical climates and occurs mainly in summer or early fall in temperate climates.
Immunity Immunity, which is type specific, may be induced by a carrier state or overt infection. In adulthood, incidence decreases markedly as immunity develops to the most prevalent serotypes. Complications ( ARA) are more common
GAS (GAS) is the most prevalent; 15% All ages 20-30% 5-18 years of age 50% During epidemics
Pathophysiology Group A beta-hemolytic streptococcal replication site in scarlet fever are the tonsils and pharynx Clinically indistinguishable, scarlet fever may follow streptococcal infection of the skin and soft tissue surgical wounds (surgical scarlet fever), or the uterus ( puerperal scarlet fever) Group A beta-hemolytic streptococci secrete a number of toxins and enzymes Erythrogenic toxin causes the pathognomonic rash of scarlet fever Local lesions reveal a characteristic inflammatory reaction, specifically hyperemia, edema, and polymorphonuclear cell infiltration.
Scarlet fever Incubation period : 1-7 days A fever of 101 degrees Fahrenheit (38.3 C) or higher . decreases 5-6 days later without AB 24 hours later Penicillin A red and sore throat that can have white or yellow patches Swollen glands in the neck Headache, throat and abdominal pain In addition to the symptoms of strep throat Nausea, and vomiting ENANTHEM: Tonsills, pharinx, tongue; edema and covered with exudate In severe cases membranous ulcers on tonsills Special appearance; 1-4 days White strawberry, 4 days later red strawberry
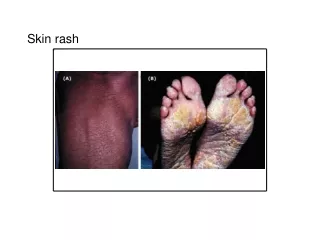
Scarlet Fever- rash A flush face with a pale area around the lips a red rash appears on the sides of chest and abdomen. It may spread to cover most of your body. This rash appears as tiny, red pinpoints and has a rough texture like sandpaper When pressed on, the rash loses color or turns white. It is redder in the creases of the elbows, arm pits, and groin areas. The rash lasts about 2-7 days. The skin on the tips of your fingers and toes often peels after rash resolves
Diagnosis Typical clinical features Isolation of agent Culture Serologic tests ( streploenzim ), ASO A rapid antigen test (“rapid strep test”) to see if there is a group A strep infection. Others: Leucocytosis Dominant PMN, %5-10 eosinophils
Treatment for scarlet fever Penicillin V oral 3-4 dose 10 days <27 kg 125 mg/dose > 27 kg 250 mg/dose Benzathine Penicillin G IM one dose <27 kg 600.000 U >27 kg 1.200.000 U Eritromycine 40 –50 mg/kg/day 3 -4 dose Amoxicillin and Ampicillin < 15 kg 125 mg/dose 3 dose > 15 kg 250 mg/dose 3 dose
Complications Early complications Cervical adenitis Otitis media Sinusitis Bronchopneumonia Rarely mastoiditis, sepsis, osteomyelitis. Late complications: 1-3 weeks later ARA ( % 3) AGN; 12,4 and 49 are nephritogenic
Late Complications Untreated group A strep infections can result in Rheumatic fever and post-streptococcal glomerulonephritis (PSGN) Rheumatic fever can develop about 18 days after a bout of strep throat and causes heart disease with or without joint pain It can be followed months later by Sydenham chorea, a disorder in which the muscles of the torso, arms, and legs move involuntarily in a dancing and jerky manner PSGN is an inflammation of the kidneys that may follow an untreated strep throat but more often comes after a strep skin infection
VARICELLA-ZOSTER VIRUS Epidemiology :Highly contagious very common between 5-10 years of age 90% infection till 10 years of age Spreads during winter and fall Droplet infection, by air way Incubation Period : 14-16 days(2-3 weeks) Transmission may occur 2 days before rash and after 7. day of rash Chicken pox is spread easily through coughs or sneezes of ill individuals, or through direct contact with secretions from the rash. Following primary infection there is usually lifelong protective immunity
Varicella-zoster virus (VZV)- chickenpox Chickenpox follows initial exposure to the virus and is typically a relatively mild, self-limited childhood illness with a characteristic exanthem Approximately 1 per 4000 children develops VZV encephalitis, an acute neurologic disorder with potentially severe complications In addition, immunocompromised children (those receiving chemotherapy for leukemia or those with advanced HIV infection) can develop disseminated VZV infection, a potentially fatal complication
Chickenpox After primary infection, VZV remains dormant in sensory nerve roots for life Upon reactivation, the virus migrates down the sensory nerve to the skin, causing the characteristic painful dermatomal rash After resolution, many individuals continue to experience pain in the distribution of the rash (postherpetic neuralgia) In addition, reactivation of VZV infection can cause a spectrum of atypical presentations, ranging from self-limited radicular pain without rash to spinal cord disease with weakness
SYMPTOMS Some kids have a fever, abdominal pain, sore throat, headache, or a vague sick feeling a day or 2 before the rash appears These symptoms may last for a few days, and fever stays in the range of 100°–102° F (37.7°–38.8° C), though in rare cases may be higher Younger kids often have milder symptoms and fewer blisters than older children or adults
Rash Chickenpox causes a red, itchy skin rash that usually appears first on the abdomen or back and face, and then spreads to almost everywhere else on the body, including the scalp, mouth, nose, ears, and genitals. The rash begins as multiple small red bumps that look like pimples or insect bites They develop into thin-walled blisters filled with clear fluid, which becomes cloudy The blister wall breaks, leaving open sores, which finally crust