Download
1 / 35
410 likes | 579 Vues
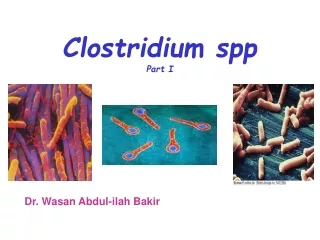
Clostridium spp Part II. Dr. Wasan Abdul-ilah Bakir Microbiology. Clostridia that produce invasive infections. C. perfringens. C. perfringens. C. perfringens is a relatively large Gram-positive short fat bacilli with blunt ends.

E N D
Clostridium spp Part II Dr. Wasan Abdul-ilah Bakir Microbiology
Clostridia that produce invasive infections C. perfringens
C. perfringens • C. perfringens is a relatively large Gram-positive short fat bacilli with blunt ends. • It is capsulate and non-motile. Anaerobic. • It grows quickly on laboratory media on blood agar. Clostridium . Perfringens In L.M Clostridium . Perfringens In E.M
C. perfringens Many different toxin-producing clostridia (C perfringens and related clostridia) can produce invasive infection (including myonecrosis and gas gangrene) if introduced into damaged tissue. About 30 species of clostridia may produce such an effect, but the most common in invasive disease is C perfringens (90%). An enterotoxin of C perfringens is a common cause of food poisoning.
C. perfringens Pathogenicity Strains of C. perfringens are widely distributed in nature, and inhabit the intestine of humans and animals. Organisms grow in traumatized tissue (especially muscle) and produce a variety of toxins. The most important is alpha toxin (lecithinase), which damages cell membranes, including those of erythrocytes, resulting in hemolysis. Derivative enzymes produce gas in tissues. C. perfringens is a member of the normal flora in the colon but not in the small bowell, where the enterotoxin acts to cause diarrhea.
C. perfringens Pathogenicity The organism produces several tissue degrading enzymes (including lecithinase [alpha toxin], proteolytic and saccharolytic enzymes). Necrosis and destruction of blood vessels and the surrounding tissue, especially muscle, result myonecrosis (is a condition of necrotic damage, specific to muscle tissue). This creates an anaerobic environment in adjacent tissue and the organism spreads systemically. C perfringens occurs in the genital tracts of 5% of women. Clostridial uterine infections followed instrumented abortions.
C. perfringens • Toxin and enzymes • The invasive clostridia produce a large variety of toxins and enzymes that result in a spreading infection. Many of these toxins have lethal, necrotizing, and hemolytic properties. • The alpha toxin of C perfringensis a lecithinase, and its lethal action at which it splits lecithin (an important constituent of cell membranes). Alpha toxin aggregates platelets, leading to formation of thrombi in small blood vessels and adding to poor tissue profusion and extending the consequences of anaerobiosis, destruction of viable tissue (gas gangrene). • Thetheta toxin has similar hemolytic and necrotizing effects but is not a lecithinase. that act by forming pores in cell membranes.
C. perfringens • Epsilon toxin is a protein that causes edema, and hemorrhage is very potent. • DNase and hyaluronidase, a collagenase that digests collagen of subcutaneous tissue and muscle. • Enterotoxin (C perfringensenterotoxin, CPE), especially when grown in meat dishes. The action ofCperfringensenterotoxin involves marked hypersecretion in the jejunum and ileum, with loss of fluids and electrolytes in diarrhea.
C. perfringens Clinical Diseases Gas gangrene the infection spreads in 1–3 days to produce crepitation in the subcutaneous tissue and muscle. Spores germinate vegetative cells multiply, ferment carbohydrates and produce gas in the tissue. This results in distension of tissue and interference with blood supply the bacteria produce lecithinase and hyaluronidase, which favor the spread of infection tissue necrosis extends, resulting in increased bacterial growth, hemolytic anemia, then severe toxemia and death.
C. perfringens Clinical Diseases Food poisoning C perfringens food poisoning usually follows the ingestion of large numbers of clostridia that have grown in warmed meat dishes. The toxin forms when the organisms sporulate in the gut, with the onset of diarrhea—usually without vomiting or fever—in 7–30 hours. The illness lasts only 1–2 days.
C. perfringens • Laboratory Diagnosis • Specimens: consist of material from wounds, pus, and tissue. • The presence of large gram-positive rods in Gram-stained smears suggests gas gangrene clostridia; spores are not regularly present. • Material is inoculated into: • Cooked meat medium ( Robertson’s medium) • Thioglycolate medium • Blood agar plates • incubated anaerobically. After pure cultures have been obtained by selecting colonies from anaerobically incubated blood plates, they are identified by biochemical reactions (various sugars in thioglycolate, action on milk), hemolysis, and colony morphology.
C. perfringens • Lecithinase activity is evaluated by the precipitate formed around colonies on egg yolk media. • Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) is a rapid and sensitive method for identification of invasive Clostridium species recovered in culture. C perfringensrarely produces spores when cultured on agar in the laboratory
C. perfringens Culture Blood agar: C. perfringens colonies exhibit a double zone of hemolysis on blood agar. C. perfringens produces raised, entire colonies with double zone hemolysis, the complete zone round the colony is due to theta toxin, and the wider zone around it is due to alpha toxin
C. perfringens • Egg Yolk Agar – Differential • Lecithinase production (white precipitate) • Lipase production (sheen around surface of colonies)
C. perfringens • Cooked meat medium ( Robertson’s medium) • It contains Meat particles (prepared from heart muscles) which contain hematin & glutathione that act as reducing agentthat absorb oxygen and allow obligate anaerobes to grow. • . • blackening of meat will observed • with the production of H2S and NH3 • Thioglycolate medium • contains beef infusion which support the growth of fastidious bacteria. Sodium thioglycollatehelps to create anaerobic conditions. Methylene blue indicates oxygen content of the medium by exhibiting a bluish-green color of the medium in the presence of oxygen
Biochemical tests: Stormy fermentationIn anaerobically-grown Litmus Milk cultures, enzymes of C. perfringens will attack the proteins and carbohydrates of the milk producing a "stormy fermentation" with acid production (the indicator, litmus turns pink), clotting of milk proteins, and gas formation.
C. perfringens Nagler's reaction for the detection of lecithinase activity A test for the identification of alpha toxin of Clostridium perfringens; the addition of antitoxin to cultures on egg yolk agar prevents visible opacity, due to lecithinase action which is normally observed around colonies. An egg-yolk plate is divided into two halves. Over one half is spread with a specific antitoxin. The culture to be tested, together with a positive control is streaked across the plate, going from the untreated area of the plate to the area that is covered with antitoxin. The culture is then incubated anaerobically. lecithinase activity, caused by the action of the Clostridium perfringens a-toxin is seen as a precipitate in the medium on the side of the plate that did not receive the antitoxin, but not on the side that was treated.
C. perfringens Nagler Reaction Procedure of Nagler Reaction Positive Nagler Reaction
C. perfringens Treatment Wounds should be débrided. Antibiotics (penicillin) administration. Hyperbaric oxygen may "detoxify" patients rapidly. C. perfringens food poisoning requires only symptomatic care.
C. perfringens Prevention and Control Early and adequate cleaning of contaminated wounds and surgical debridement, together with the administration of antimicrobial drugs directed against clostridia (eg, penicillin), are the best available preventive measures.
Clostridium difficile and diarrheal disease C. difficile
C. difficile C. difficile is responsible for antibiotic-associated gastrointestinal disease ranging from self-limited diarrhea to severe, life threatening psudomembranous colitis. It is a part of normal intestinal flora in a small number of healthy people and hospitalized patients. The spores can contaminate an environment for many months and can be a major source of nosocomial outbreaks.
C. difficile • Pseudomembranous Colitis • Administration of antibiotics results in proliferation of drug-resistant C difficilethat produces two toxins: • Toxin A, a potent enterotoxin that also has some cytotoxic activity, binds to the brush border membranes of the gut at receptor sites. • Toxin B is a potent cytotoxin. • The results is apoptosis, capillary leakage, cytokine stimulation, and other consequences that lead to colitis. • Not all strains of C difficileproduce the toxins, and the toxin genes are found on a large, chromosomal pathogenicity island along with three other genes that regulate toxin expression. Although many antibiotics have been associated with pseudomembranous colitis, the most common are ampicillin and clindamycin and, more recently, the fluoroquinolones
C. difficile C difficile causes diarrhea associated with yellow- white Plaques on the colonic mucosa. Fever and abdominal pain often occur. The pseudomembranes are visualized by sigmoidoscopy.
C. difficile Laboratory Diagnosis Pseudomembranous colitis is diagnosed by: 1. detection of one or both C difficile toxins in stool by isolation of C. difficile in the feces and detection of toxins with tissue culture cells (cytotoxicity assay). 2. endoscopic observation of pseudomembranes or microabscesses in patients who have diarrhea and have been given antibiotics. Plaques and microabscesses may be localized to one area of the bowel. The diarrhea may be watery or bloody, and the patient frequently has associated abdominal cramps, leukocytosis, and fever.
C. difficile • Treatment • The disease is treated by: • discontinuing administration of the offending antibiotic and orally giving metronidazole, vancomycin, or fidaxomicin. • 2. Fecal transplantation has become a successful and routine method for recurrent and refractory disease. This usually involves administration of the feces of a healthy related donor by way of colonoscopy or less commonly via a nasogastric tube into the gastrointestinal tract of the patient.
C. difficile Fecal transplantation
Antibiotic-Associated Diarrhea The administration of antibiotics frequently leads to a mild to moderate form of diarrhea, termed antibiotic-associated diarrhea. This disease is generally less severe than the classic form of pseudomembranous colitis. As many as 25% of cases of antibiotic-associated diarrhea are caused by C difficile infection. Other Clostridium species such as C perfringens and C sordellii have also been implicated. The latter two species are not associated with pseudomembranous colitis.
C. septicum is a cause of nontraumatic myonecrosis and frequently exists in patients with occult colon cancer, acute leukemia, and diabetes. It can spread from GI tract into tissue and result in fulminant infection with high mortality within 1 to 2 days.