Download
1 / 38
400 likes | 699 Vues
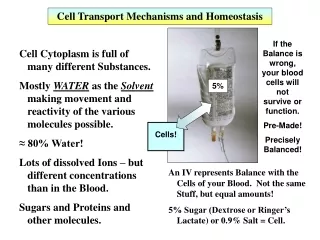
Renal Transport Mechanisms. Renal Physiology 4 09/19/2012 Charles J. Foulks, M.D. GFR 125 ml/min (180L/day) (about 1% is excreted). Filtration, reabsoption , and excretion rates of substances by the kidneys Filtered Reabsorbed Excreted Reabsorbed

E N D
Renal Transport Mechanisms Renal Physiology 4 09/19/2012 Charles J. Foulks, M.D.
GFR 125 ml/min (180L/day) • (about 1% is excreted)
Filtration, reabsoption, and excretion rates of substances by the kidneys Filtered Reabsorbed Excreted Reabsorbed (meq/24h) (meq/24h) (meq/24h) (%) Glucose (g/day) 180 180 0 100 Bicarbonate (meq/day) 4,320 4,318 2 > 99.9 Sodium (meq/day) 25,560 25,410 150 99.4 Chloride (meq/day) 19,440 19,260 180 99.1 Water (l/day) 169 167.5 1.5 99.1 Urea (g/day) 48 24 24 50 Creatinine (g/day) 1.8 0 1.8 0
Two pathways of the absorption: Transcellular Pathway Paracellular transport Plasma Lumen Cells
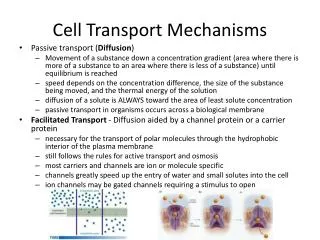
Mechanism of Transport 1. Primary Active Transport 2. Secondary Active Transport 3. Pinocytosis 4. Passive Transport
Primary active reabsorption 1- Na+ diffuse across basolateralmemb by Na+ -K+ pump 2- Na+ diffuses across luminal memb into the cell according to electro chemical gradient established by Na+ -K+ pump 3- Na+, water & other substances are reabsorbed into peritubular capillaries
Secondary active reabsorption Co transport • 2 substances bind to a specific carrier protein • E.g. Na+ diffuses down electrochemical gradient & glucose is transported against its chemical gradient in luminal border • No direct energy from ATP but it depends on energy of primary active Na+ - K+ pump
Passive reabsorption It occurs secondary to solute reabsorption Chloride -follows Na reabsorption -PCT& DCT Water By osmosis to interstitium through paracellular route Bicarbonate formed inside the cell from carbonic acids by the help of carbonic anhyderase Urea Reabsorped secondary to water reabsorption
Pinocytosis: Some parts of the tubule, especially the proximal tubule, reabsorb large molecules such as proteins by pinocytosis.
Transportation of Sodium, Water and Chloride Sodium, water and chloride reabsorption in proximal tubule Proximal tubule, including the proximal convoluted tubule and thick descending segment of the loop Proximal reabsorption is ISOMOTIC. The PT is the Arnold Schwarzennger of the kidney.
Tubular secretion Transport of substances from peritubular capillaries to tubular lumen Primary active secretion -For H+ -In late distal & collecting tubules -H+ -ATPase pump at luminal memb Secondary active secretion -H+ in PCT (counter-transport) -K+, urate in distal tubules
Reabsorption & secretion along different parts of the nephtron The proximal convoluted tubule PCT Reabsorption of • 65% of Na+ ( 1ry active) • 65 % of K+ (2ry active), water, urea & Cl- (passive) • 100% of glucose & amino acids ( 2ry active) • 90% Ca • Po4 , Mg+, nitrate, sulfate • Bicarbonate formed inside the cell from carbonic acids by the help of carbonic anhyderase to give HCO3&H2 HCO3 is reabsorbed &H2 is secreted
Secretion • H2 (2ry active counter transport - antiport) • Ammonia formed inside the tubular cells acts as H2 acceptor • Waste products & drugs
Reabsorb about 65 percent of the filtered sodium, chloride, bicarbonate, and potassium and essentially al the filtered glucose and amino acids. Secrete organic acids, bases, and hydrogen ions into the tubular lumen.
Sodium, water and chloride reabsorption in proximal tubule The sodium-potassium ATPase: major force for reabsorption of sodium, chloride and water In the first half of the proximal tubule, sodium is reabsorbed by co-transport along with glucose, amino acids, and other solutes. In the second half of the proximal tubule, sodium reabsorbed mainly with chloride ions.
Sodium, water and chloride reabsorption in proximal tubule The second half of the proximal tubule has a relatively high concentration of chloride (around 140mEq/L) compared with the early proximal tubule (about 105 mEq/L) In the second half of the proximal tubule, the higher chloride concentration favors the diffusion of this ion from the tubule lumen through the intercellular junctions into the renal interstitial fluid. Early PT reabsorbs bicarbonate which is gone by late PT.
Na+ absorption • Na+ absorbed by active transport mechanisms, NOT by TM mechanism. Basolateral ATPases establish a gradient across the tubule wall. • Proximal tubule is very permeable to Na+, so ions flow down gradient, across membranes. • Microvilli create large surface area for absorption. • Electrical gradient created also draws Cl- across. • H2O follows Na+ due to osmotic force. • Means fluid left in tubule is concentrated.
(2) Sodium and water transport in the loop of Henle The loop of Henle consists of three functionally distinct segments: the thin descending segment, the thin ascending segment, and the thick ascending segment.
TDLH High permeable to water and moderately permeable to most solutes but has few mitochondria and little or no active reabsorption. TALH Reabsorbs about 25% of the filtered loads of sodium, chloride, and potassium, as well as large amounts of calcium, bicarbonate, and magnesium. This segment also secretes hydrogen ions into the tubule
Mechanism of sodium, chloride, and potassium transport in the thick ascending loop of Henle
K+ handling • K+ is major cation in cells and balance is essential for life. • Small change from 4 to 5.5 mmoles/l = hyperkalaemia = ventric. fibrillation = death. • To 3.5 mmoles/l = hyperpolarise = arrhythmias and paralysis = death. • Reabsorb K+ at proximal tubule. • Changes in K+ excretion due to changes in K+ secretion in distal tubule • Medullary trapping of K+ helps to maximise K+ excretion when K+ intake is high.
K+ handling • K+reabsorption along the proximal tubule is largely passive and follows the movement of Na+ and fluid (in collecting tubules, may also rely active transport). • K+secretion occurs in cortical collecting tubule (principal cells), and relies upon active transport of K+ across basolateral membrane and passive exit across apical membrane into tubular fluid.
2. Glucose Reabsorption Glucose is reabsorbed along with Na+ in the early portion of the proximal tubule. Glucose is typical of substances removed from the urine by secondary active transport. Essentially all of the glucose is reabsorbed, and no more than a few milligrams appear in the urine per 24 hours.
The amount reabsorbed is proportionate to the amount filtered and hence to the plasma glucose level (PG) times the GFR up to the transport maximum (TmG); But when the TmG is exceed, the amount of glucose in the urine rises The TmG is about 375 mg/min in men and 300 mg/min in women.
GLUCOSE REABSORPTION HAS A TUBULAR MAXIMUM Glucose Reabsorbed mg/min Excreted Filtered Reabsorbed Renal threshold (300mg/100 ml) Plasma Concentration of Glucose
The renal threshold for glucose is the plasma level at which the glucose first appears in the urine. One would predict that the renal threshold would be about 300 mg/dl – ie, 375 mg/min (TmG) divided by 125 mL/min (GFR). However, the actual renal threshold is about 200 mg/dL of arterial plasma, which corresponds to a venous level of about 180 mg/dL.
Top: Relationship between the plasma level (P) and excretion (UV) of glucose and inulin Bottom: Relationship between the plasma glucose level (PG) and amount of glucose reabsorbed (TG).
Glucose handling • Glucose absorption also relies upon the Na+ gradient. • Most reabsorbed in proximal tubule. • At apical membrane, needs Na+/glucose cotransporter (SGLT) • Crosses basolateral membrane via glucose transporters (GLUT’s), which do not rely upon Na+.
Amino acid handling • Preserve as much of these essential nutrients as possible. • Can be absorbed by GI tract, products of protein catabolism, or de novo synthesis of nonessential amino acids. • TM values lower than that of glucose, so can excrete excess in urine. • Amino acid transporters rely upon Na+ gradient at apical membrane, but a couple of exceptions don’t. • Exit across basolateral membrane via diffusion , but again, some exceptions rely on Na+.
1. Reabsorption is a 2-step process: lumen to interstitium, and interstitium to peritubular capillary. 2. Flux from lumen to interstitium can be transcellular, using separate transport steps in the apical and basolateral membranes, or paracellular, around the cells through tight junctions. 3. Channels and transporters promote the transmembrane flux of solutes that cannot permeate lipid bilayers. 4. Osmotic gradients drive a volume flux across membranes and epithelia.
5. Osmotic pressure and osmolality mean the same thing and represent the power of dissolved solute to drive an osmotic flux of water. • 6. For convenience, osmolality is approximated by the easier concept of osmolarity. • 7. Water and solutes, which are reabsorbed from lumen to interstitium, • then move from interstitium to peritubular capillaries by bulk flow, • driven by Starling forces. • 8. The reabsorption of water and almost all solutes is linked, directly or • indirectly, to the active reabsorption of sodium. • 9. All reabsorptive processes have a limit on how fast they can occur, • either because the transporters saturate (Tm systems) or because the • substance leaks back into the lumen (gradient-limited systems)